

Association of Elevated Amyloid and Tau Positron Emission Tomography Signal With Near-Term Development of Alzheimer Disease Symptoms in Older Adults Without Cognitive Impairment
- PMID: 35907254
- PMCID: PMC9339146
- DOI: 10.1001/jamaneurol.2022.2379
Association of Elevated Amyloid and Tau Positron Emission Tomography Signal With Near-Term Development of Alzheimer Disease Symptoms in Older Adults Without Cognitive Impairment
Abstract
Importance: National Institute on Aging-Alzheimer's Association (NIA-AA) workgroups have proposed biological research criteria intended to identify individuals with preclinical Alzheimer disease (AD).
Objective: To assess the clinical value of these biological criteria to identify older individuals without cognitive impairment who are at near-term risk of developing symptomatic AD.
Design, setting, and participants: This longitudinal cohort study used data from 4 independent population-based cohorts (PREVENT-AD, HABS, AIBL, and Knight ADRC) collected between 2003 and 2021. Participants were older adults without cognitive impairment with 1 year or more of clinical observation after amyloid β and tau positron emission tomography (PET). Median clinical follow-up after PET ranged from 1.94 to 3.66 years.
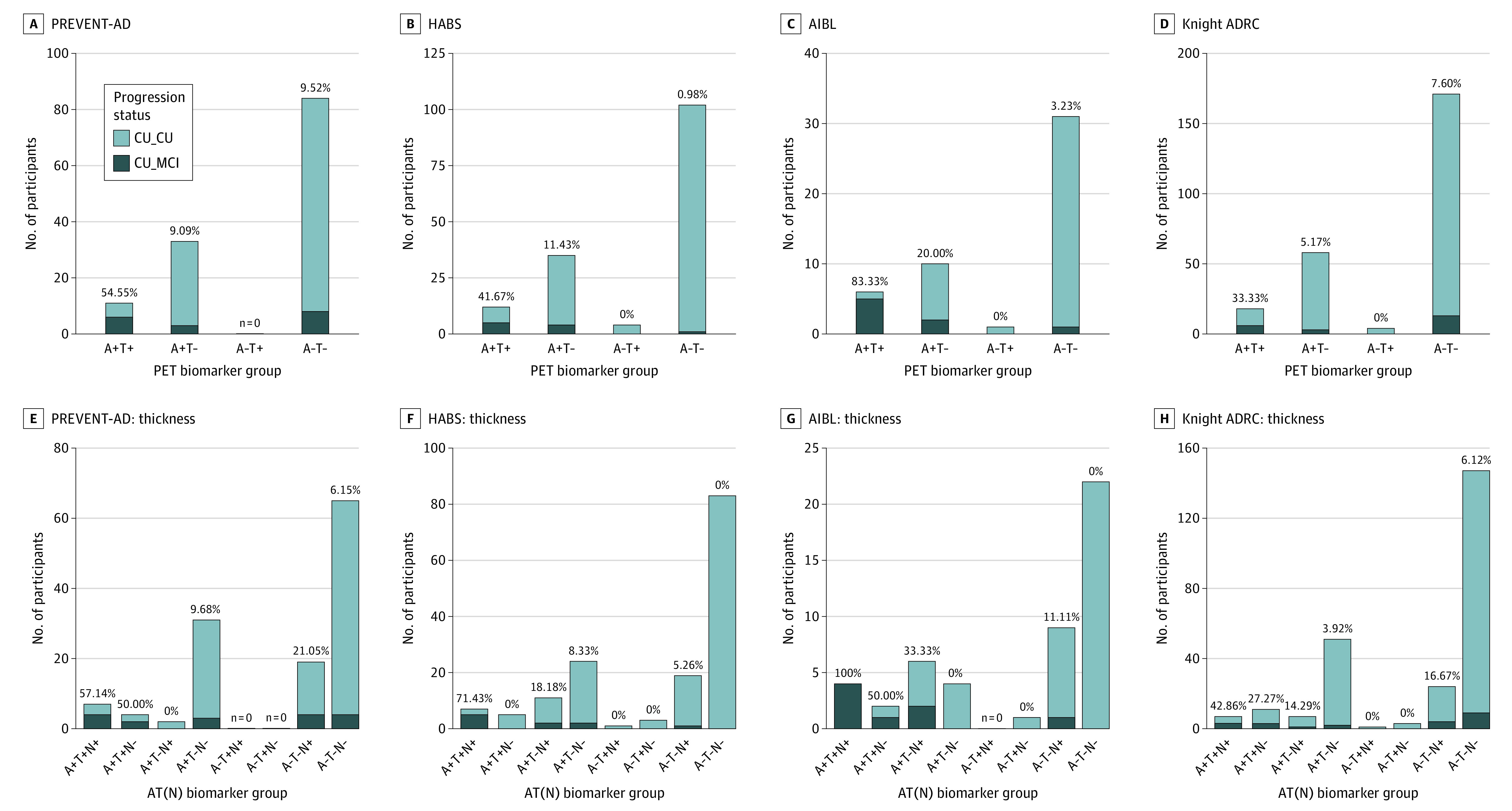
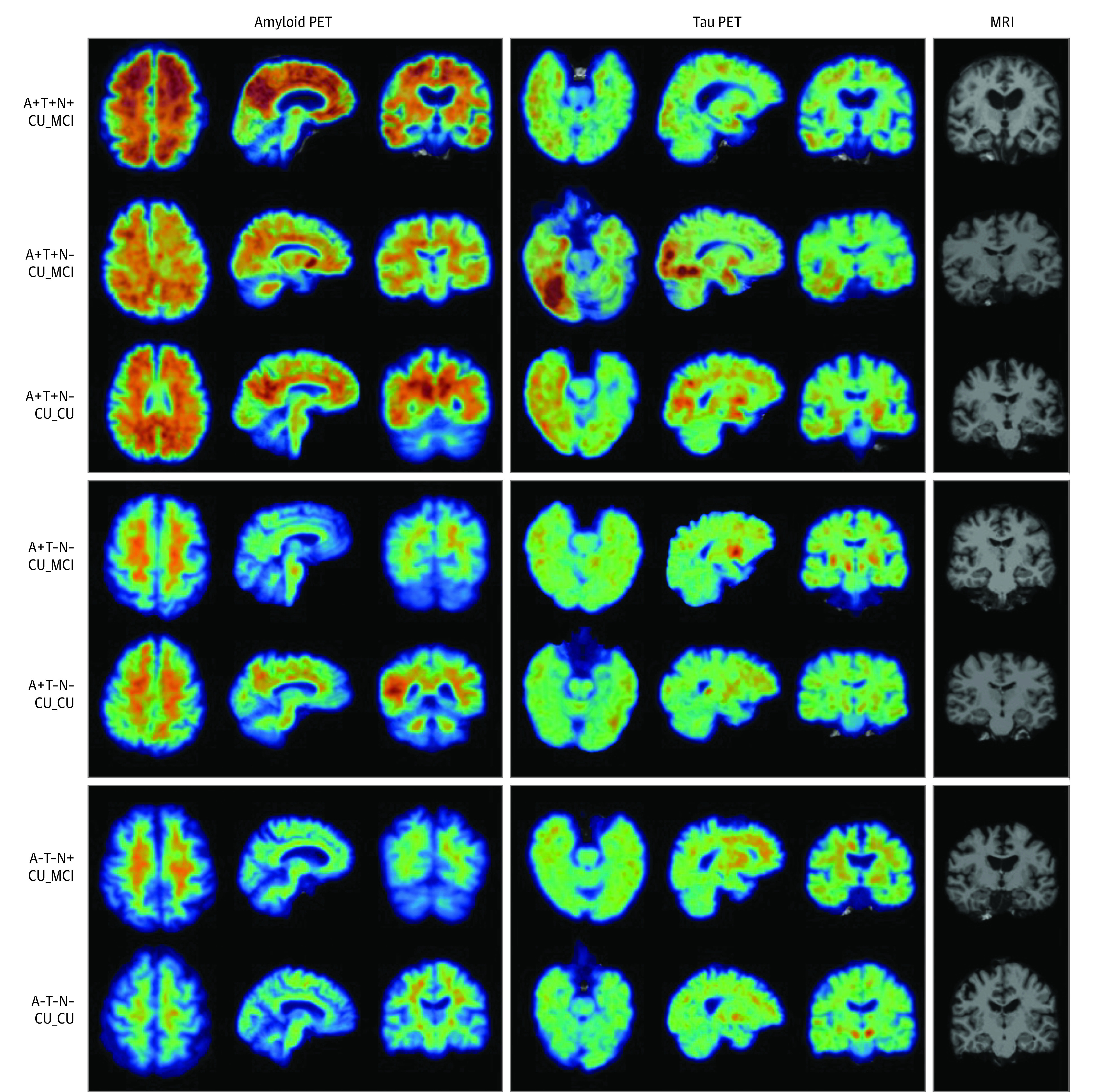
Exposures: Based on binary assessment of global amyloid burden (A) and a composite temporal region of tau PET uptake (T), participants were stratified into 4 groups (A+T+, A+T-, A-T+, A-T-). Presence (+) or absence (-) of neurodegeneration (N) was assessed using temporal cortical thickness.
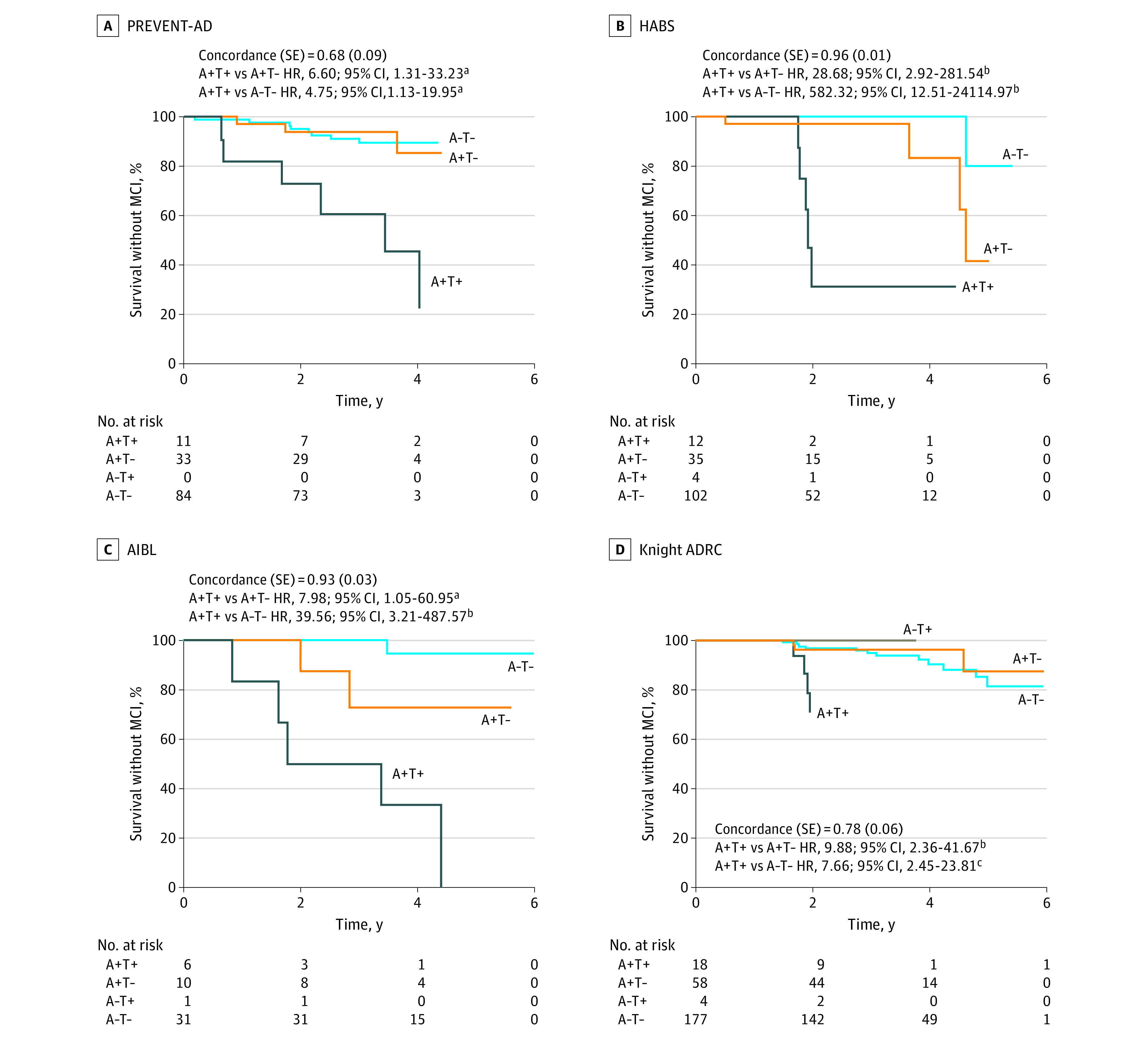
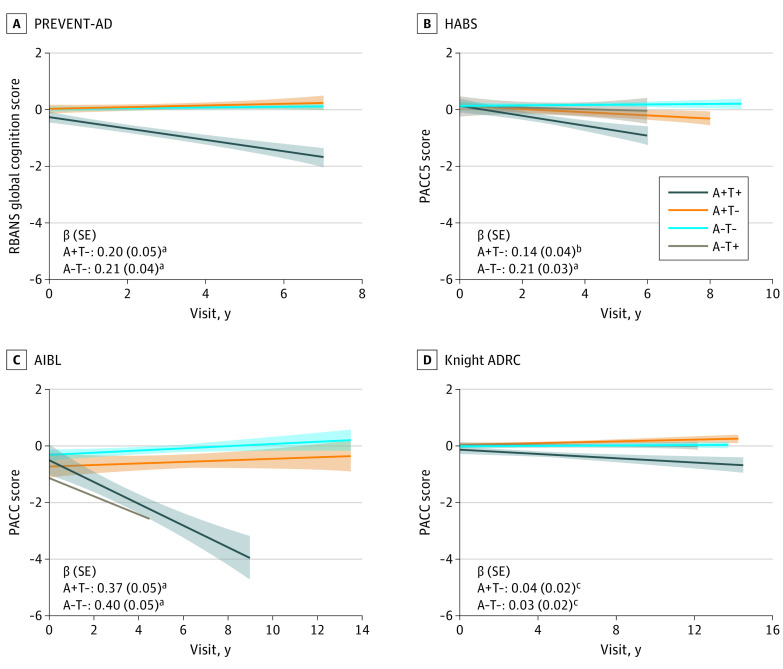
Main outcomes and measures: Each cohort was analyzed separately. Primary outcome was clinical progression to mild cognitive impairment (MCI), identified by a Clinical Dementia Rating score of 0.5 or greater in Knight ADRC and by consensus committee review in the other cohorts. Clinical raters were blind to imaging, genetic, and fluid biomarker data. A secondary outcome was cognitive decline, based on a slope greater than 1.5 SD below the mean of an independent subsample of individuals without cognitive impairment. Outcomes were compared across the biomarker groups.
Results: Among 580 participants (PREVENT-AD, 128; HABS, 153; AIBL, 48; Knight ADRC, 251), mean (SD) age ranged from 67 (5) to 76 (6) years across cohorts, with between 55% (137/251) and 74% (95/128) female participants. Across cohorts, 33% to 83% of A+T+ participants progressed to MCI during follow-up (mean progression time, 2-2.72 years), compared with less than 20% of participants in other biomarker groups. Progression further increased to 43% to 100% when restricted to A+T+(N+) individuals. Cox proportional hazard ratios for progression to MCI in the A+T+ group vs other biomarker groups were all 5 or greater. Many A+T+ nonprogressors also showed longitudinal cognitive decline, while cognitive trajectories in other groups remained predominantly stable.
Conclusions and relevance: The clinical prognostic value of NIA-AA research criteria was confirmed in 4 independent cohorts, with most A+T+(N+) older individuals without cognitive impairment developing AD symptoms within 2 to 3 years.
Conflict of interest statement
Figures
Comment in
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
