

Acute kidney injury associated to COVID-19 leads to a strong unbalance of circulant immune mediators
- PMID: 35907365
- PMCID: PMC9309102
- DOI: 10.1016/j.cyto.2022.155974
Acute kidney injury associated to COVID-19 leads to a strong unbalance of circulant immune mediators
Abstract
Background: Severe cases of coronavirus disease 2019 (COVID-19) have increased risk for acute kidney injury (AKI). The exacerbation of the immune response seems to contribute to AKI development, but the immunopathological process is not completely understood.
Objectives: To analyze levels of circulant immune mediators in COVID-19 patients evolving with or without AKI. We have also investigated possible associations of these mediators with viral load and clinical outcomes.
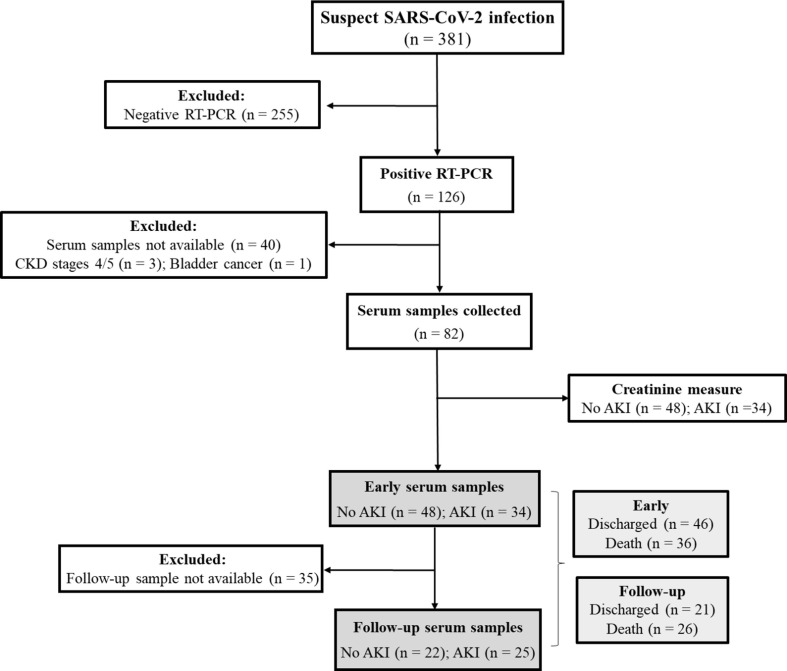
Methods: This is a longitudinal study performed with hospitalized patients with moderate to severe COVID-19. Serum levels of 27 immune mediators were measured by a multiplex immunoassay. Data were analyzed at two timepoints during the follow-up: within the first 13 days of the disease onset (early sample) and from the 14th day to death or hospital discharge (follow-up sample).
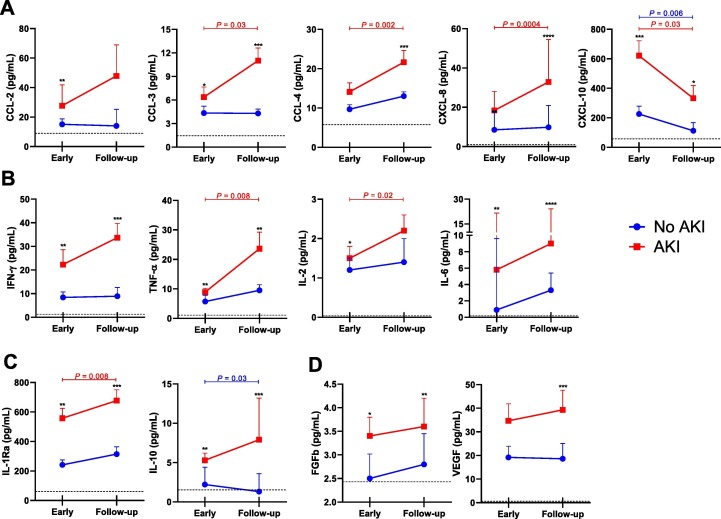
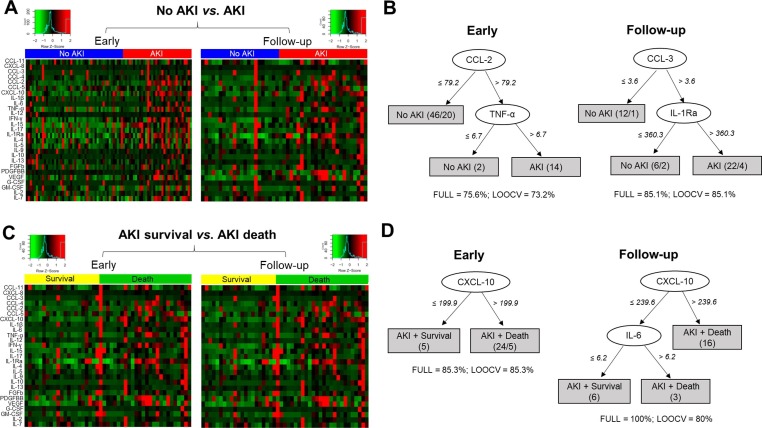
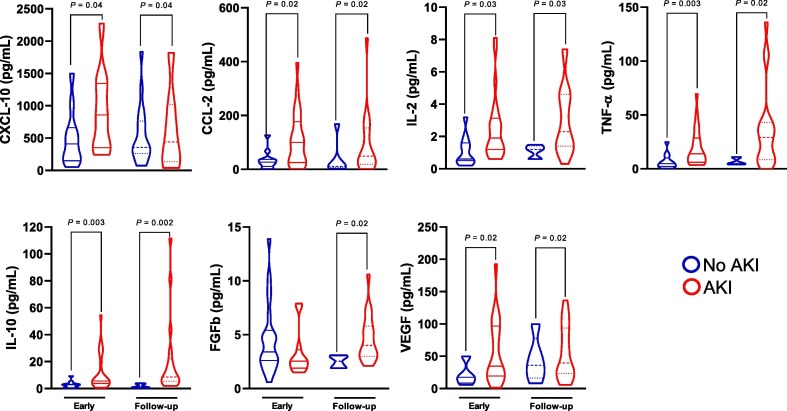
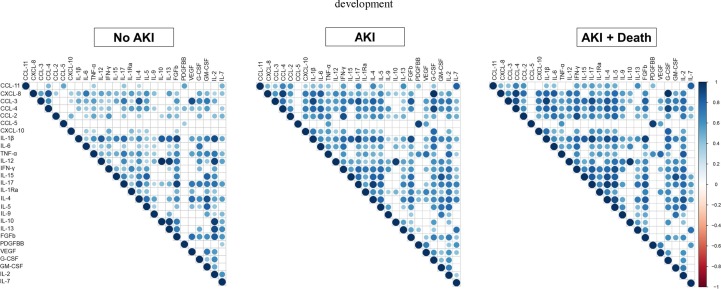
Results: We studied 82 COVID-19 patients (59.5 ± 17.5 years, 54.9% male). Of these, 34 (41.5%) developed AKI. These patients presented higher SARS-CoV-2 viral load (P = 0.03), higher frequency of diabetes (P = 0.01) and death (P = 0.0004). Overall, AKI patients presented significantly higher and sustained levels (P < 0.05) of CCL-2, CCL-3, CCL-4, CXCL-8, CXCL-10, IFN-γ, IL-2, IL-6, TNF-α, IL-1Ra, IL-10 and VEGF. Importantly, higher levels of CCL-2, CXCL-10, IL-2, TNF-α, IL-10, FGFb, and VEGF were observed in AKI patients independently of death. ROC curves demonstrated that early alterations in CCL-2, CXCL-8, CXCL-10, IFN-γ, IL-6, IL-1Ra and IL-10 show a good predictive value regarding AKI development. Lastly, immune mediators were significantly associated with each other and with SARS-CoV-2 viral load in AKI patients.
Conclusions: COVID-19 associated AKI is accompanied by substantial alterations in circulant levels of immune mediators, which could significantly contribute to the establishment of kidney injury.
Keywords: Acute kidney injury; COVID-19; Cytokines; Immune mediators.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
CCL-2 and CXCL-8: Potential Prognostic Biomarkers of Acute Kidney Injury after a Bothrops atrox Snakebite.Mediators Inflamm. 2022 Sep 7;2022:8285084. doi: 10.1155/2022/8285084. eCollection 2022. Mediators Inflamm. 2022. PMID: 36117588 Free PMC article.
-
Longitudinal COVID-19 profiling associates IL-1RA and IL-10 with disease severity and RANTES with mild disease.JCI Insight. 2020 Jul 9;5(13):e139834. doi: 10.1172/jci.insight.139834. JCI Insight. 2020. PMID: 32501293 Free PMC article.
-
Antimicrobial peptides and other potential biomarkers of critical illness in SARS-CoV-2 patients with acute kidney injury. AMPAKI-CoV study.Physiol Rep. 2024 Feb;12(3):e15945. doi: 10.14814/phy2.15945. Physiol Rep. 2024. PMID: 38328863 Free PMC article.
-
Adaptive immunity to SARS-CoV-2 infection: A systematic review.Front Immunol. 2022 Oct 10;13:1001198. doi: 10.3389/fimmu.2022.1001198. eCollection 2022. Front Immunol. 2022. PMID: 36300105 Free PMC article.
-
Pathophysiology and Clinical Manifestations of COVID-19-Related Acute Kidney Injury-The Current State of Knowledge and Future Perspectives.Int J Mol Sci. 2021 Jun 30;22(13):7082. doi: 10.3390/ijms22137082. Int J Mol Sci. 2021. PMID: 34209289 Free PMC article. Review.
Cited by
-
Global geographic and socioeconomic disparities in COVID-associated acute kidney injury: a systematic review and meta-analysis.J Glob Health. 2025 Jul 25;15:04166. doi: 10.7189/jogh.15.04166. J Glob Health. 2025. PMID: 40709582 Free PMC article.
-
Exploring Urinary Extracellular Vesicles and Immune Mediators as Biomarkers of Kidney Injury in COVID-19 Hospitalized Patients.Diagnostics (Basel). 2022 Oct 27;12(11):2600. doi: 10.3390/diagnostics12112600. Diagnostics (Basel). 2022. PMID: 36359444 Free PMC article.
-
The role of CXCL family members in different diseases.Cell Death Discov. 2023 Jul 1;9(1):212. doi: 10.1038/s41420-023-01524-9. Cell Death Discov. 2023. PMID: 37393391 Free PMC article. Review.
-
The Role of Extracellular Vesicles in SARS-CoV-2-Induced Acute Kidney Injury: An Overview.Life (Basel). 2024 Jan 23;14(2):163. doi: 10.3390/life14020163. Life (Basel). 2024. PMID: 38398672 Free PMC article. Review.
-
The multifaceted nature of IL-10: regulation, role in immunological homeostasis and its relevance to cancer, COVID-19 and post-COVID conditions.Front Immunol. 2023 Jun 8;14:1161067. doi: 10.3389/fimmu.2023.1161067. eCollection 2023. Front Immunol. 2023. PMID: 37359549 Free PMC article. Review.
References
-
- Gao Y., Ding M., Dong X., Zhang J., Kursat Azkur A., Azkur D., et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy. 2021 Feb;76(2):428–455. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
