

The prevalence of alcoholic and nonalcoholic fatty liver disease in adolescents and young adults in the United States: analysis of the NHANES database
- PMID: 35907827
- PMCID: PMC9338651
- DOI: 10.1186/s12876-022-02430-7
The prevalence of alcoholic and nonalcoholic fatty liver disease in adolescents and young adults in the United States: analysis of the NHANES database
Abstract
Background: The prevalence of fatty liver disease is potentially increasing in adolescents and young adults (AYAs) due to the obesity and alcohol pandemics. The aim of this study was to assess the prevalence of alcohol-associated fatty liver disease (ALD) and nonalcoholic fatty liver disease (NAFLD) in a representative U.S. cohort utilizing transient elastography to directly measure hepatic steatosis and suspected fibrosis.
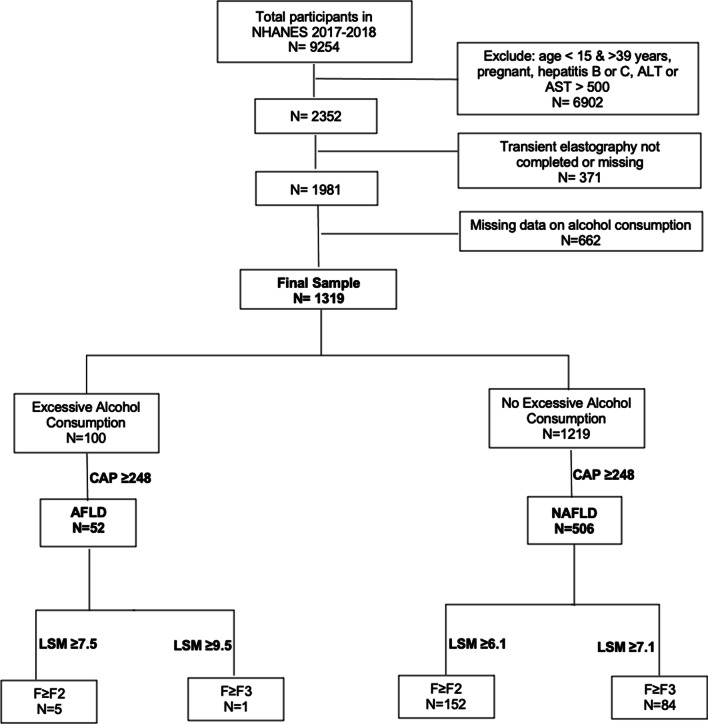
Methods: AYAs (age 15-39 years) with valid FibroScan® measurements in the National Health and Nutrition Examination Survey (NHANES) database (2017-2018) were included in the analyses. Those with viral hepatitis, pregnancy, or ALT/AST > 500 U/L were excluded. The population was divided into those with excessive alcohol consumption (ALQ130) and those without. Controlled attenuation parameter (CAP) score ≥ 248 dB/m was used to identify suspected ALD and NAFLD. In those with evidence of ALD, the following cutoffs of liver stiffness measurement (LSM) were used for suspected fibrosis: F ≥ F2 at LSM ≥ 7.5 kPa and F ≥ F3 at ≥ 9.5 kPa, respectively. In those with suspected NAFLD, the following LSM cutoffs were used: F ≥ F2 at 6.1 and F ≥ F3 at ≥ 7.1, respectively. Cutoffs were chosen based on published literature to maximize sensitivity.
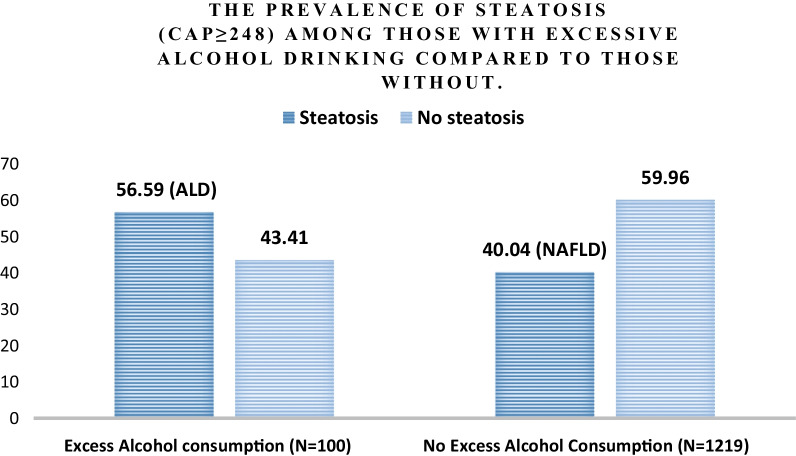
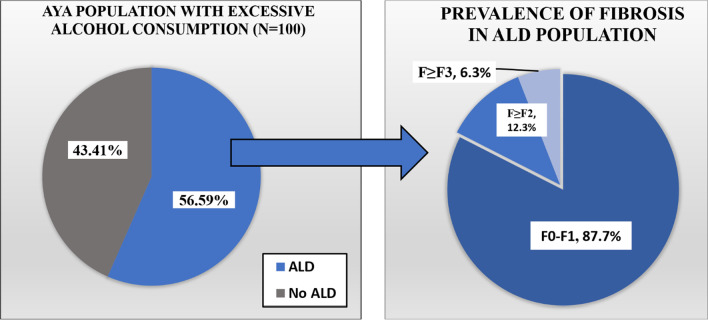
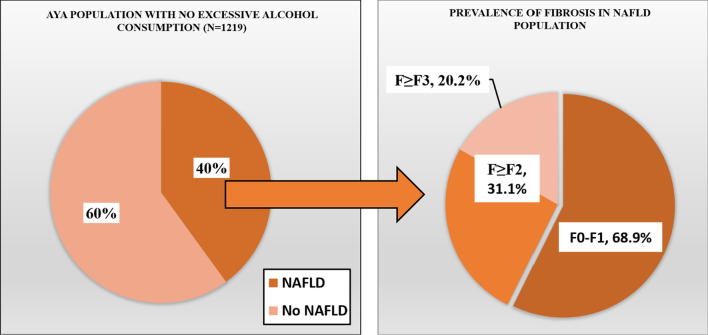
Results: Comparing to those without, subjects with excessive alcohol consumption tended to be older (29.8 vs 28.5 years), have a higher BMI (29.3 vs 28.9 kg/m2), and be from a White ethnicity (65.3% vs. 55.4%). In subjects with excessive alcohol consumption, suspected ALD was present in 56.59% (95% CI 41.57-70.49). In those with suspected ALD, suspected significant fibrosis (F ≥ F2) was present in 12.3% (95% CI 4.74-28.34) and advanced fibrosis (F ≥ F3) was present in 6.31% (95% CI 0.69-39.55). Similarly, in subjects without excessive alcohol consumption, suspected NAFLD was present in 40.04% (36.64-43.54). In those with suspected NAFLD, suspected significant fibrosis (F ≥ F2) was present in 31.07% (27.25-35.16) and suspected advanced fibrosis (F ≥ F3) was present in 20.15% (16.05-24.99).
Conclusion: A significant percentage of AYAs are at risk for ALD and NAFLD and a subset of these subjects is at risk for significant fibrosis. Efforts should focus on increasing awareness of the prevalence of ALD and NAFLD in this population and to mitigate modifiable risk factors.
Keywords: ALD; Alcohol; Cirrhosis; Elastography; Fibroscan; Fibrosis; NAFLD.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
