

Mitigating structural racism to reduce inequities in sepsis outcomes: a mixed methods, longitudinal intervention study
- PMID: 35907839
- PMCID: PMC9338573
- DOI: 10.1186/s12913-022-08331-5
Mitigating structural racism to reduce inequities in sepsis outcomes: a mixed methods, longitudinal intervention study
Abstract
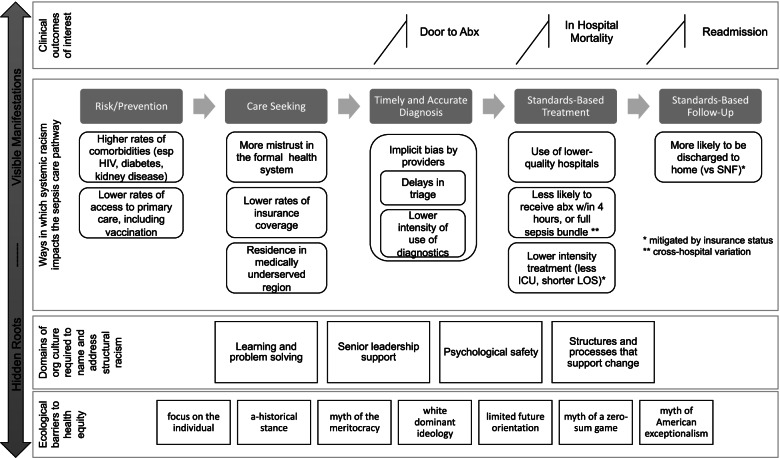
Background: Sepsis affects 1.7 million patients in the US annually, is one of the leading causes of mortality, and is a major driver of US healthcare costs. African American/Black and LatinX populations experience higher rates of sepsis complications, deviations from standard care, and readmissions compared with Non-Hispanic White populations. Despite clear evidence of structural racism in sepsis care and outcomes, there are no prospective interventions to mitigate structural racism in sepsis care, nor are we aware of studies that report reductions in racial inequities in sepsis care as an outcome. Therefore, we will deliver and evaluate a coalition-based intervention to equip health systems and their surrounding communities to mitigate structural racism, driving measurable reductions in inequities in sepsis outcomes. This paper presents the theoretical foundation for the study, summarizes key elements of the intervention, and describes the methodology to evaluate the intervention.
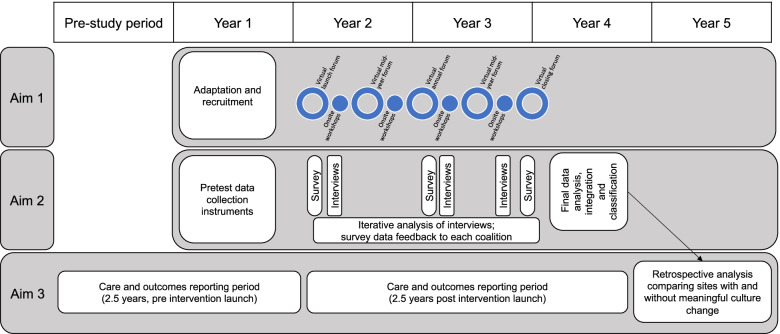
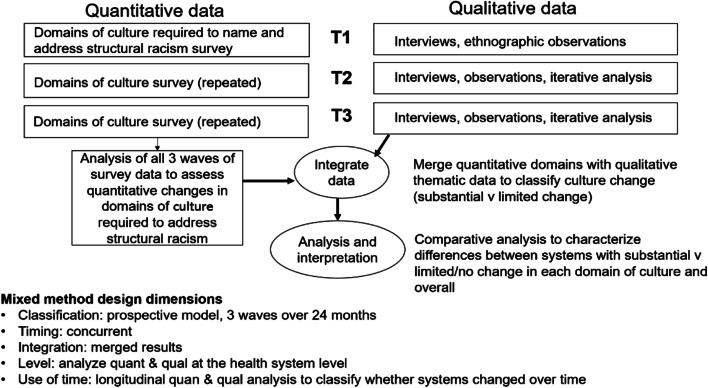
Methods: Our aims are to: (1) deliver a coalition-based leadership intervention in eight U.S. health systems and their surrounding communities; (2) evaluate the impact of the intervention on organizational culture using a longitudinal, convergent mixed methods approach, and (3) evaluate the impact of the intervention on reduction of racial inequities in three clinical outcomes: a) early identification (time to antibiotic), b) clinical management (in-hospital sepsis mortality) and c) standards-based follow up (same-hospital, all-cause sepsis readmissions) using interrupted time series analysis.
Discussion: This study is aligned with calls to action by the NIH and the Sepsis Alliance to address inequities in sepsis care and outcomes. It is the first to intervene to mitigate effects of structural racism by developing the domains of organizational culture that are required for anti-racist action, with implications for inequities in complex health outcomes beyond sepsis.
Keywords: Health Systems; Intervention Studies; Leadership; Organizational Culture; Racial Disparities; Sepsis; Structural Racism.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Hall MJ, Levant S, DeFrances CJ. Trends in inpatient hospital deaths: national hospital discharge survey, 2000-2010. NCHS Data Brief. 2013;(118):1–8. - PubMed
