

Evaluating the effectiveness of abbreviated breast MRI (abMRI) interpretation training for mammogram readers: a multi-centre study assessing diagnostic performance, using an enriched dataset
- PMID: 35907862
- PMCID: PMC9338668
- DOI: 10.1186/s13058-022-01549-5
Evaluating the effectiveness of abbreviated breast MRI (abMRI) interpretation training for mammogram readers: a multi-centre study assessing diagnostic performance, using an enriched dataset
Abstract
Background: Abbreviated breast MRI (abMRI) is being introduced in breast screening trials and clinical practice, particularly for women with dense breasts. Upscaling abMRI provision requires the workforce of mammogram readers to learn to effectively interpret abMRI. The purpose of this study was to examine the diagnostic accuracy of mammogram readers to interpret abMRI after a single day of standardised small-group training and to compare diagnostic performance of mammogram readers experienced in full-protocol breast MRI (fpMRI) interpretation (Group 1) with that of those without fpMRI interpretation experience (Group 2).
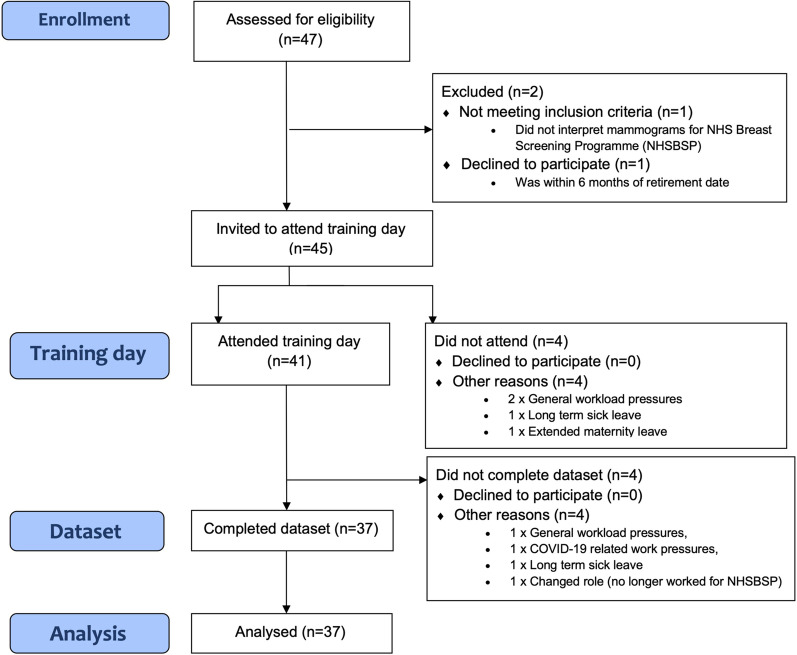
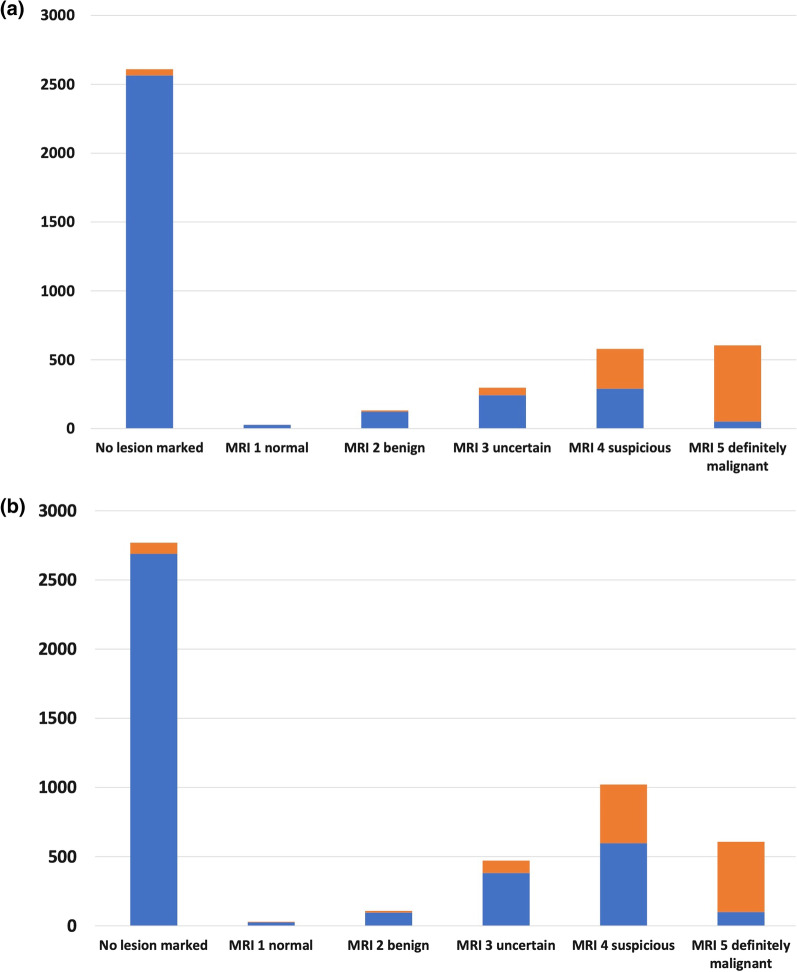
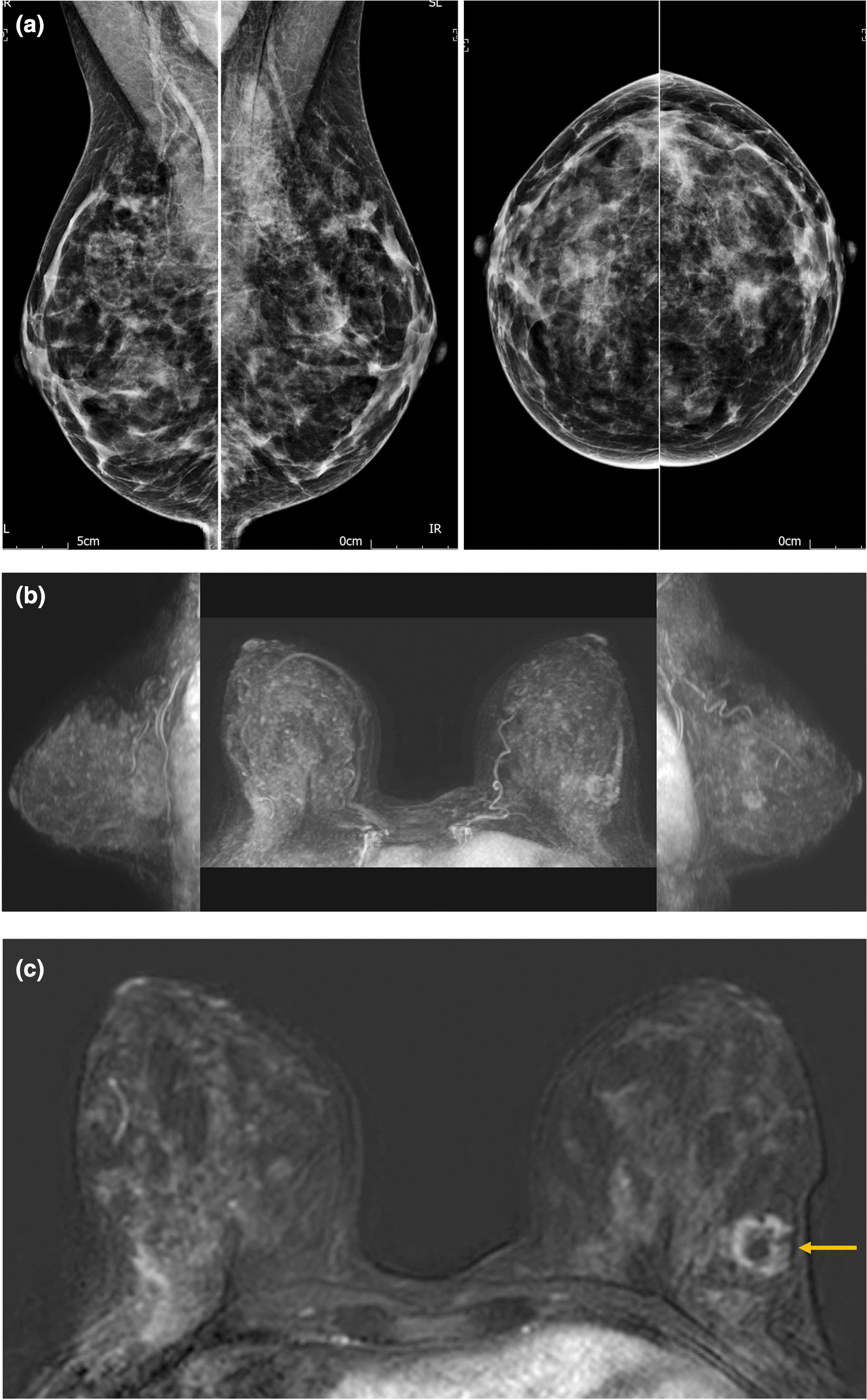
Methods: Mammogram readers were recruited from six NHS Breast Screening Programme sites. Small-group hands-on workstation training was provided, with subsequent prospective, independent, blinded interpretation of an enriched dataset with known outcome. A simplified form of abMRI (first post-contrast subtracted images (FAST MRI), displayed as maximum-intensity projection (MIP) and subtracted slice stack) was used. Per-breast and per-lesion diagnostic accuracy analysis was undertaken, with comparison across groups, and double-reading simulation of a consecutive screening subset.
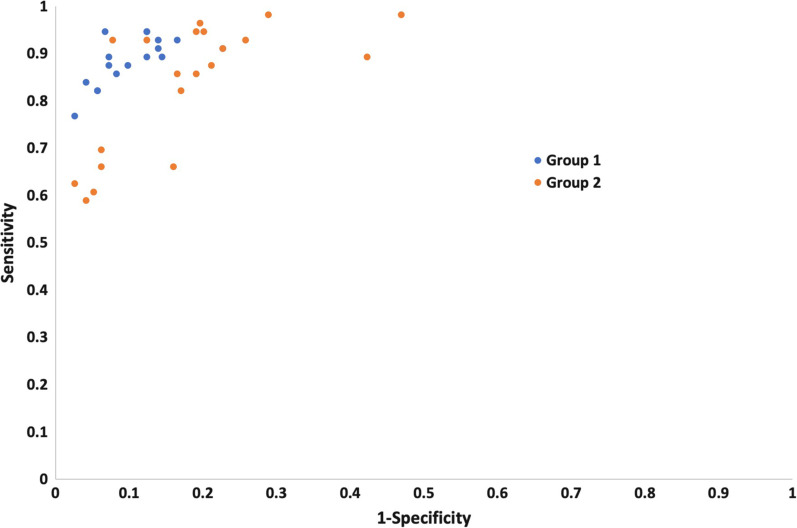
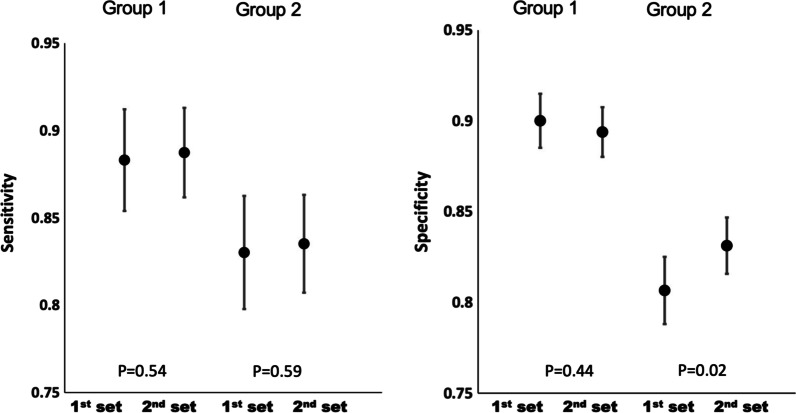
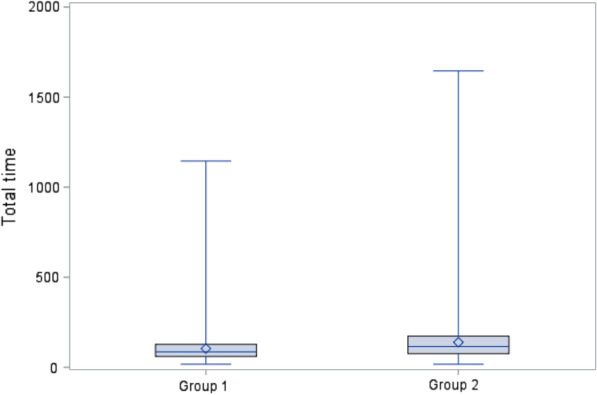
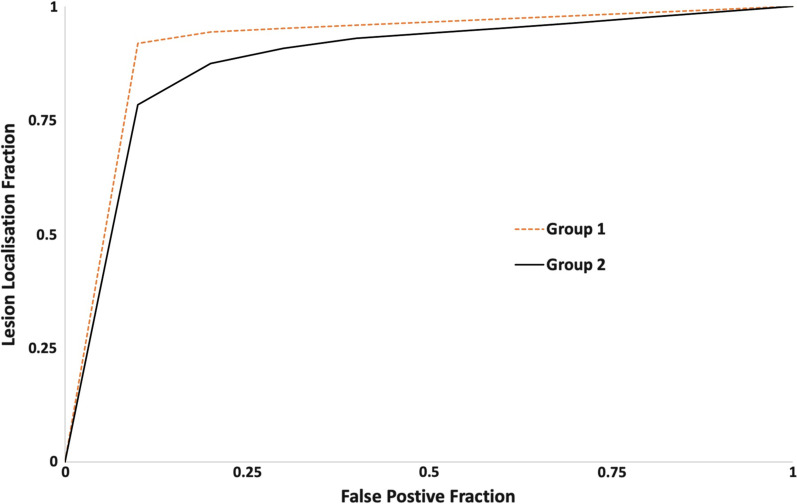
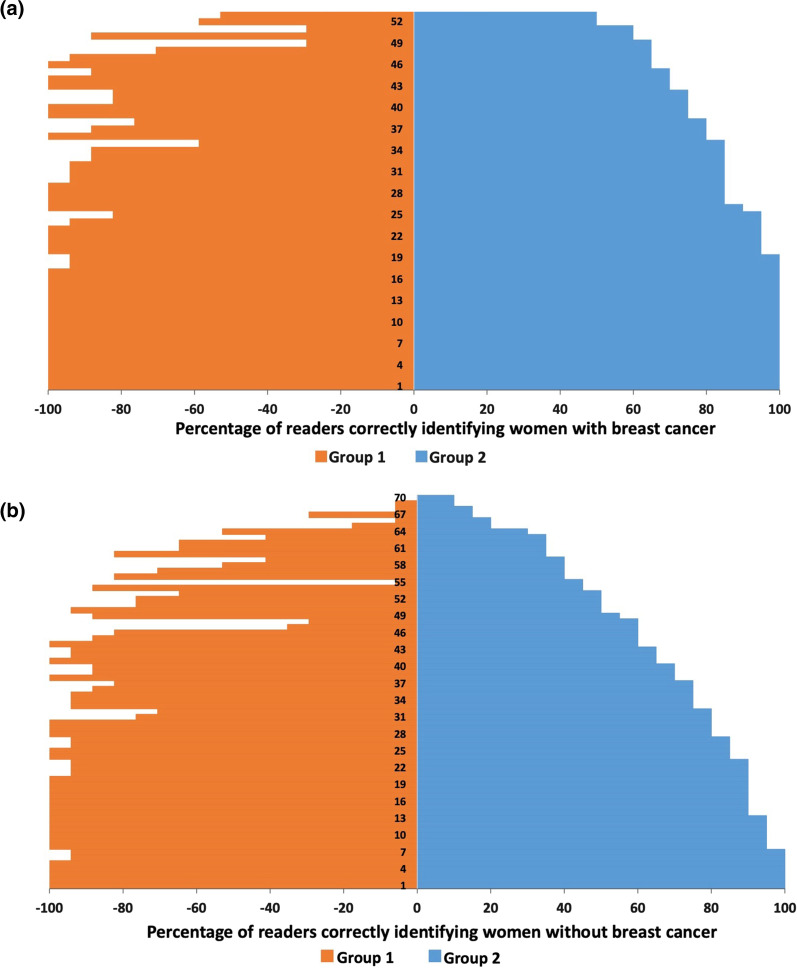
Results: 37 readers (Group 1: 17, Group 2: 20) completed the reading task of 125 scans (250 breasts) (total = 9250 reads). Overall sensitivity was 86% (95% confidence interval (CI) 84-87%; 1776/2072) and specificity 86% (95%CI 85-86%; 6140/7178). Group 1 showed significantly higher sensitivity (843/952; 89%; 95%CI 86-91%) and higher specificity (2957/3298; 90%; 95%CI 89-91%) than Group 2 (sensitivity = 83%; 95%CI 81-85% (933/1120) p < 0.0001; specificity = 82%; 95%CI 81-83% (3183/3880) p < 0.0001). Inter-reader agreement was higher for Group 1 (kappa = 0.73; 95%CI 0.68-0.79) than for Group 2 (kappa = 0.51; 95%CI 0.45-0.56). Specificity improved for Group 2, from the first 55 cases (81%) to the remaining 70 (83%) (p = 0.02) but not for Group 1 (90-89% p = 0.44), whereas sensitivity remained consistent for both Group 1 (88-89%) and Group 2 (83-84%).
Conclusions: Single-day abMRI interpretation training for mammogram readers achieved an overall diagnostic performance within benchmarks published for fpMRI but was insufficient for diagnostic accuracy of mammogram readers new to breast MRI to match that of experienced fpMRI readers. Novice MRI reader performance improved during the reading task, suggesting that additional training could further narrow this performance gap.
Keywords: Abbreviated breast MRI; Breast cancer; Diagnostic accuracy; Education; FAST MRI; Training.
© 2022. The Author(s).
Conflict of interest statement
Other than the funding sources declared above, the authors declare that they have no other competing interests.
Figures
References
-
- Comstock CE, Gatsonis C, Newstead GM, Snyder BS, Gareen IF, Bergin JT, et al. Comparison of abbreviated breast MRI vs digital breast tomosynthesis for breast cancer detection among women with dense breasts undergoing screening. JAMA J Am Med Assoc. 2020;323(8):746–56. doi: 10.1001/jama.2020.0572. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
