

An analysis of alternative forced oscillation technique reporting and validation methods for within- and between-sessions in healthy adults
- PMID: 35907930
- PMCID: PMC9338972
- DOI: 10.1038/s41598-022-17264-2
An analysis of alternative forced oscillation technique reporting and validation methods for within- and between-sessions in healthy adults
Abstract
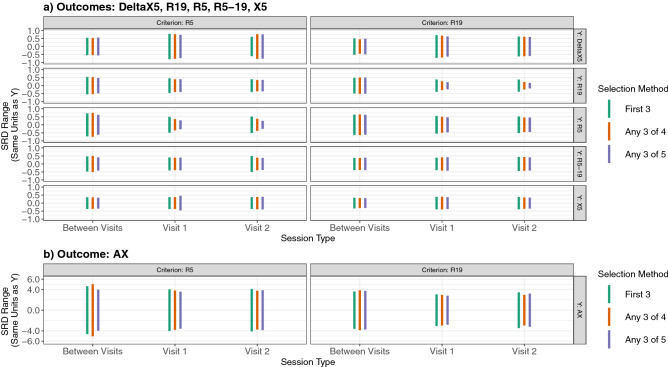
Forced oscillation technique (FOT) provides unique information on respiratory system mechanical properties complementing pulmonary function testing. However, a lack of evidence guiding acquisition/reporting of parameters has slowed clinical FOT adoption. Current European Respiratory Society (ERS) standards recommend 3-5 trials per session comprising three trials with a coefficient of variation (CoV) ≤ 10% for low-frequency resistance. We present an analysis of different combinations of trial selection methods and session validity thresholding variables (low- and mid-frequency resistance and reactance [R5, R19, X5], low-frequency reactance area [AX] and tidal volume) comparing proportion of subjects achieving valid data across two test sessions (7 ± 3 days apart) and within and between session measurement variabilities. 126 (98%) subjects achieved valid data across both sessions (2666 trials). With R5 or R19 as criteria and selection of any three trials from ≥ 4 attempts, ≥ 75% of subjects achieved validity. Furthermore, with R5 or R19 criteria and selection of any trials from ≥ 5 attempts, CoVs for resistance outcomes were reduced within session while variabilities of FOT outcomes between sessions remained consistent. Within session differences in measurement variabilities were not clinically meaningful. Our analyses support current ERS reporting recommendations for healthy adults. Future work should apply this analytic approach to patient populations.
© 2022. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
