

Consensus statement on the current pharmacological prevention and management of heart failure
- PMID: 35908234
- PMCID: PMC9545515
- DOI: 10.5694/mja2.51656
Consensus statement on the current pharmacological prevention and management of heart failure
Abstract
Introduction: This consensus statement of Australian clinicians provides new recommendations for the pharmacological management of heart failure based on studies reported since the publication of the 2018 Australian heart failure guidelines.
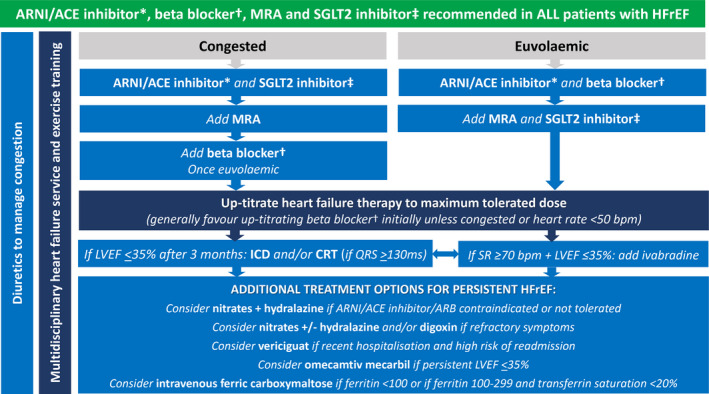
Main recommendations: ▪Use of sodium-glucose cotransporter 2 (SGLT2) inhibitors to prevent hospitalisation for heart failure in type 2 diabetes mellitus can be extended to patients with multiple cardiovascular risk factors, albuminuric chronic kidney disease, or atherosclerotic cardiovascular disease. ▪New evidence supports the use of a mineralocorticoid receptor antagonist (finerenone) to prevent heart failure in type 2 diabetes mellitus associated with albuminuric chronic kidney disease. ▪In addition to renin angiotensin system inhibitors (angiotensin receptor neprilysin inhibitor preferred), beta blockers and mineralocorticoid receptor antagonists, an SGLT2 inhibitor (dapagliflozin or empagliflozin) is recommended in all patients with heart failure with reduced left ventricular ejection fraction (LVEF ≤ 40%) (HFrEF). Lower quality evidence supports these therapies in patients with heart failure with mildly reduced LVEF (41-49%) (HFmrEF). ▪A soluble guanylate cyclase stimulator (vericiguat), selective cardiac myosin activator (omecamtiv mecarbil) and, if iron deficient, intravenous iron (ferric carboxymaltose) provide additional benefits in persistent HFrEF. ▪An SGLT2 inhibitor (empagliflozin) should be considered in patients with heart failure with preserved LVEF (≥ 50%) (HFpEF). Key changes in management from this statement: This document broadens the scope of angiotensin receptor neprilysin inhibitor use in patients with HFrEF and HFmrEF. SGLT2 inhibitor use expands to become a cornerstone therapy in HFrEF, with increasing evidence to support its use in HFmrEF and HFpEF.
Keywords: Cardiomyopathies; Guidelines as topic; Heart failure.
© 2022 The Authors. Medical Journal of Australia published by John Wiley & Sons Australia, Ltd on behalf of AMPCo Pty Ltd.
Conflict of interest statement
All authors were supported by the South Australian Health and Medical Research Institute for the initial heart failure consensus statement conference. We were offered an honorarium to attend the virtual meeting by the Evidence to Practice Group. No other funding was provided. Andrew Sindone reports consultancy fees, speaking honoraria or research support from Amgen, AstraZeneca, Bayer, Biotronik, Boehringer Ingelheim, Bristol Myers Squibb, Menarini, Merck Sharp and Dohm, Mylan, Novartis, Otsuka, Pfizer, Sanofi, Servier, and Vifor. Carmine De Pasquale reports consultancy fees, speaking honoraria or research support from AstraZeneca, Novartis, Vifor, Boehringer Ingelheim, Bayer, Lily, Roche Diagnostics, and American Regent. John Amerena reports consultancy fees, speaking honoraria, conference and research support from AstraZeneca, Novartis, Vifor, Boehringer Ingelheim, Bayer, Lilly, and Amgen. Christine Burdeniuk reports consultancy fees and speaking honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, and Novartis. Alicia Chan reports speaking honoraria or research support from Novartis, AstraZeneca, Boehringer Ingelheim, Vifor, Medtronic, Biotronik, Abbott, and Boston Scientific. Andrew Coats reports consultancy fees, speaking honoraria or research support from AstraZeneca, Boehringer Ingelheim, Menarini, Novartis, Servier, Vifor, Abbott, Actimed, Arena, Cardiac Dimensions, Corvia, CVRx, Enopace, ESN Cleer, Faraday, Impulse Dynamics, Respicardia, and Viatris. David Hare reports research grants, consultancy fees and speaking honoraria from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Lundbeck, Menarini, Merck, Novartis, Pfizer, Sanofi, Servier, and Vifor. Peter Macdonald reports peer‐reviewed research funding from the National Health and Medical Research Council and NSW Health, industry‐supported research funding to his institution from Amgen and Novartis, and consultancy fees paid to him from AstraZeneca, Boehringer Ingelheim, and Novartis. Aaron Sverdlov is supported by National Heart Foundation of Australia Future Leader Fellowships (Award IDs 101918 and 106025) and reports research grants from the NSW Health, Hunter Medical Research Institute, Biotronik, RACE Oncology, Bristol Myer Squibb, Roche Diagnostics, and Vifor; and consultancy fees and speaking honoraria from Novartis, Bayer, Bristol Myer Squibb, AstraZeneca, and Boehringer Ingelheim. John Atherton reports consultancy fees, speaking honoraria or research support from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Lilly, and Novartis.
Figures
References
-
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021; 42: 3599‐3726. - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2022; 79: e263‐e421. - PubMed
-
- Atherton JJ, Sindone A, De Pasquale CG, et al. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the management of heart failure 2018. Med J Aust 2018; 209: 363‐369. https://www.mja.com.au/journal/2018/209/8/national‐heart‐foundation‐aust... - PubMed
-
- Atherton JJ, Sindone A, De Pasquale CG, et al. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: guidelines for the prevention, detection, and management of heart failure in Australia 2018. Heart Lung Circ 2018; 27: 1123‐1208. - PubMed
-
- Schünemann HBJ, Guyatt G, Oxman A, editors. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. Updated October 2013. https://gdt.gradepro.org/app/handbook/handbook.html (viewed Apr 2022).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
