

Decision-making in stereotactic epilepsy surgery
- PMID: 35908245
- PMCID: PMC9669234
- DOI: 10.1111/epi.17381
Decision-making in stereotactic epilepsy surgery
Abstract
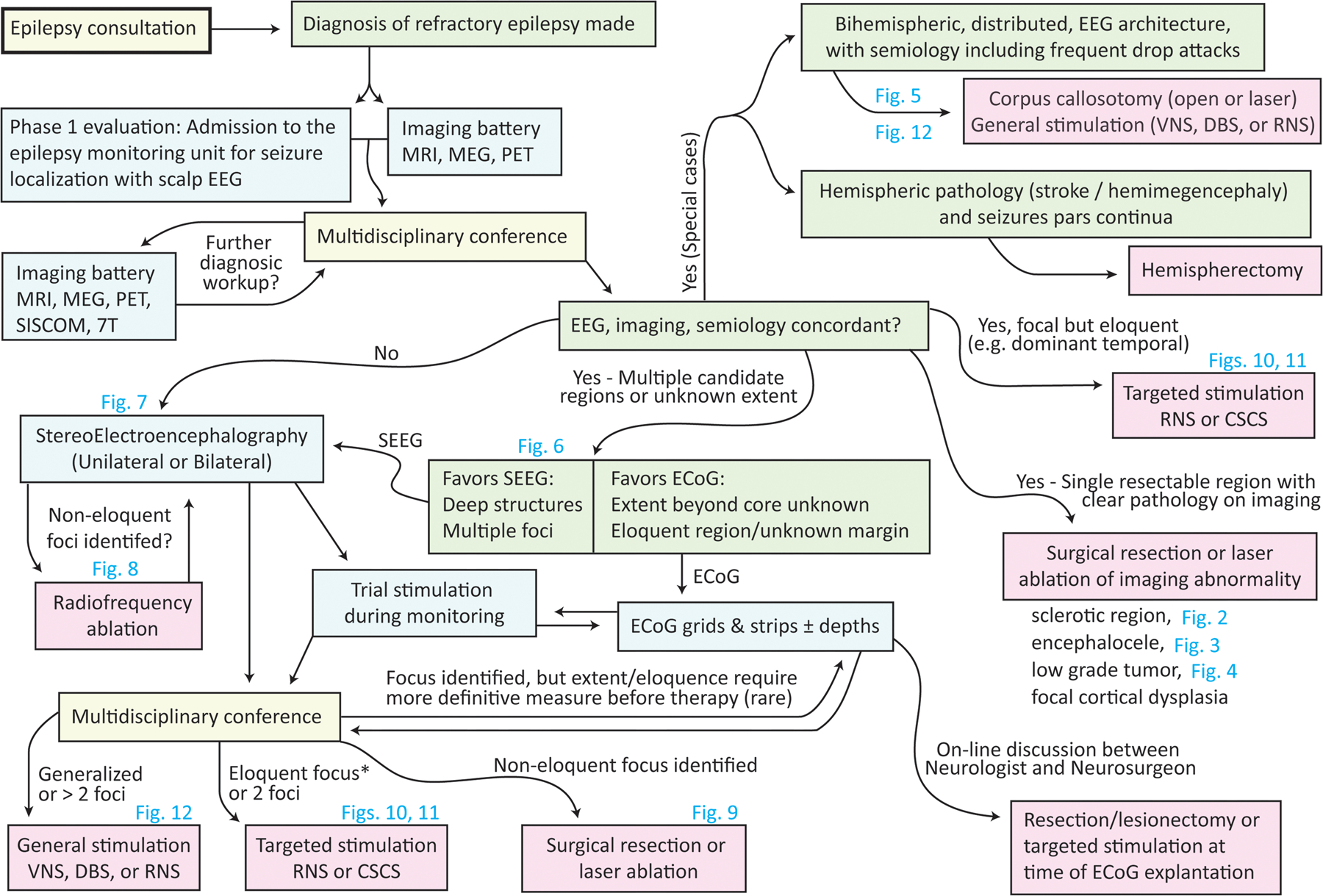
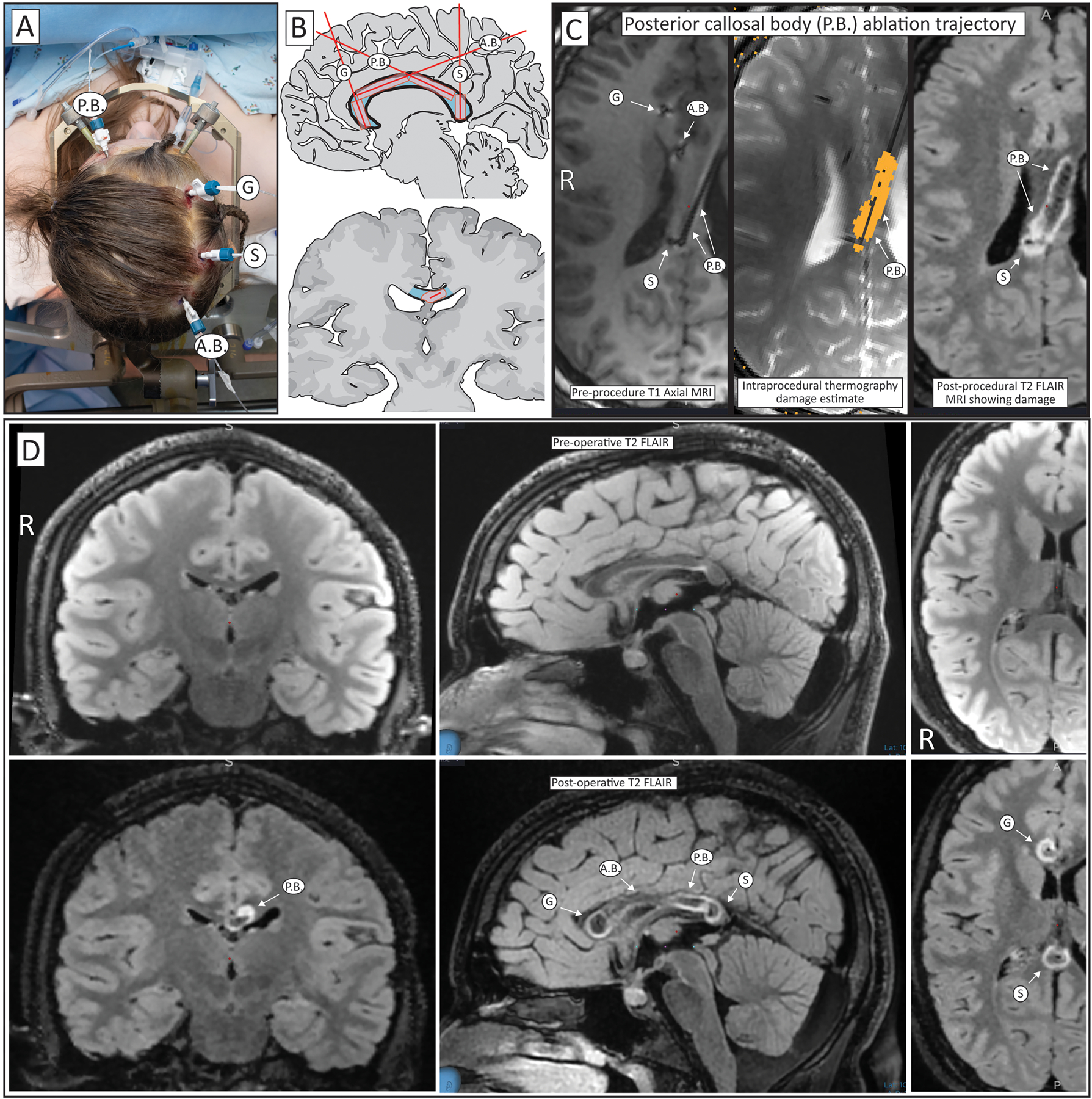
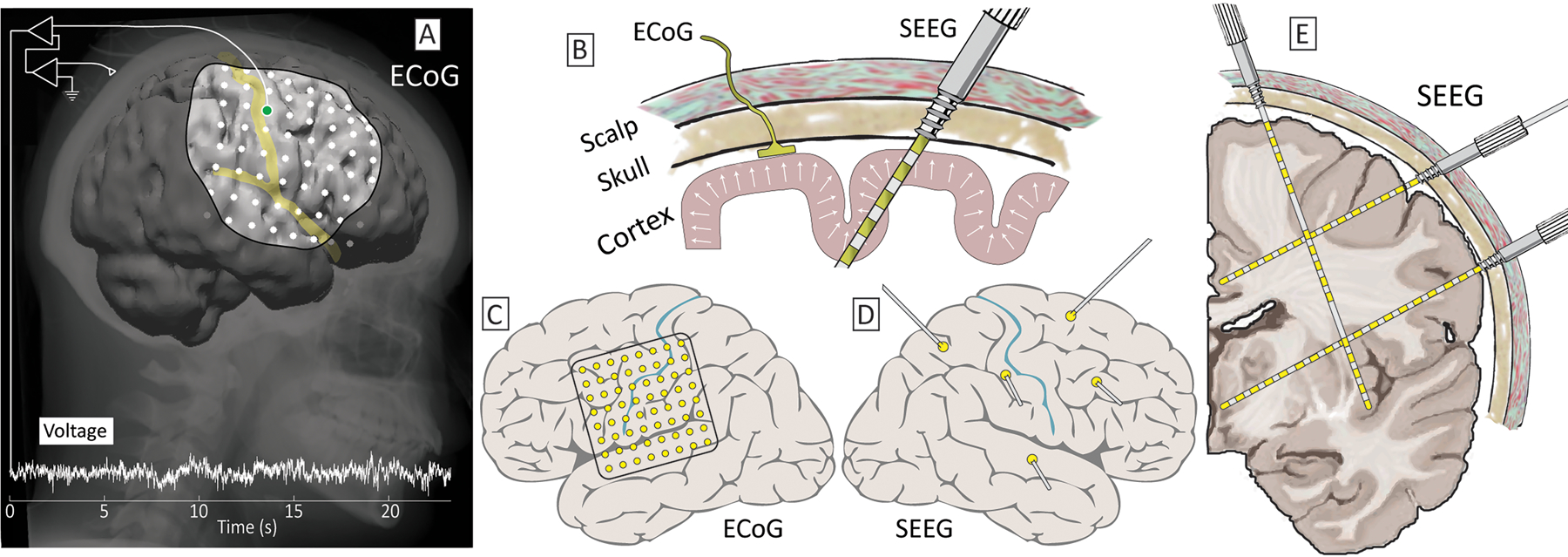
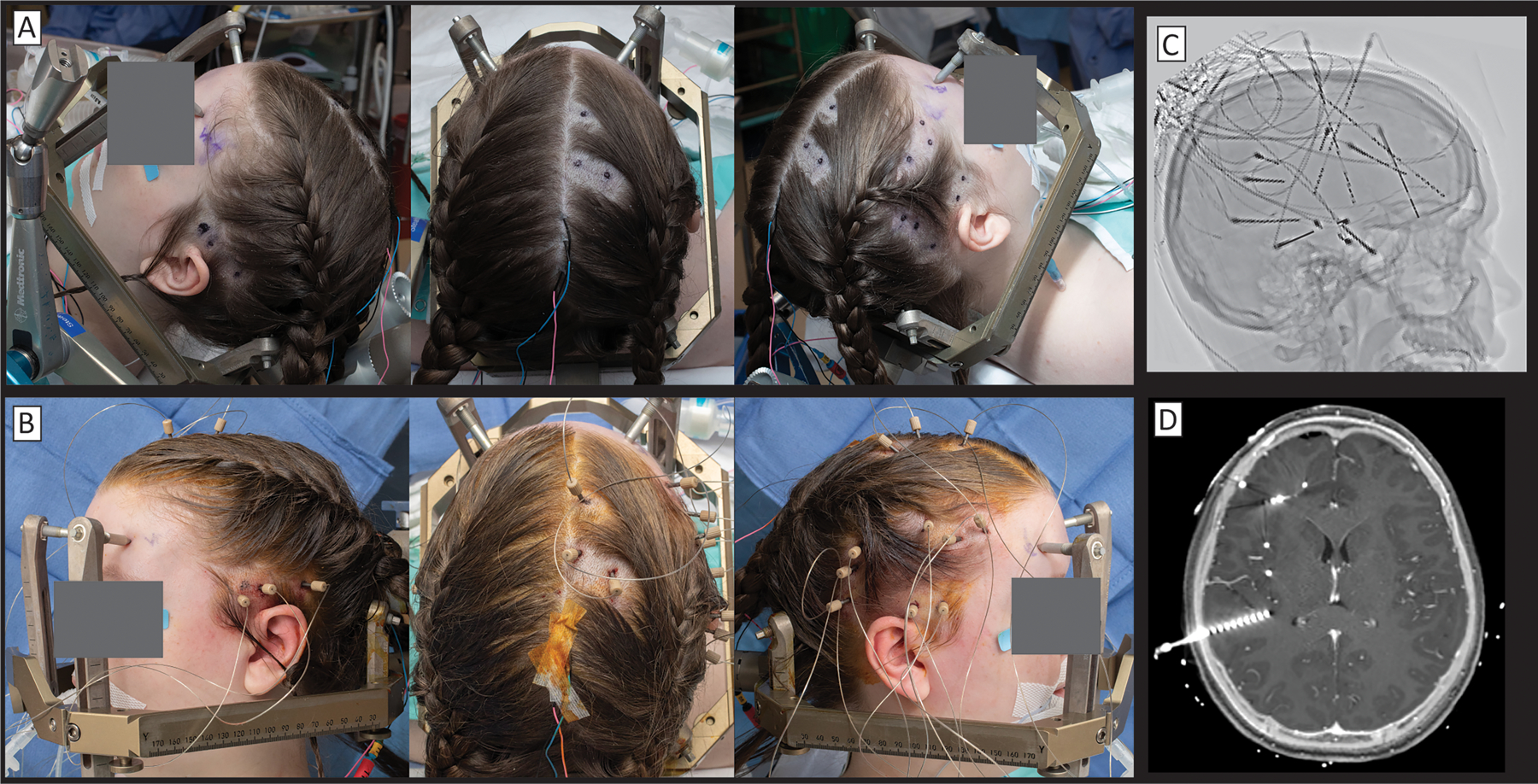
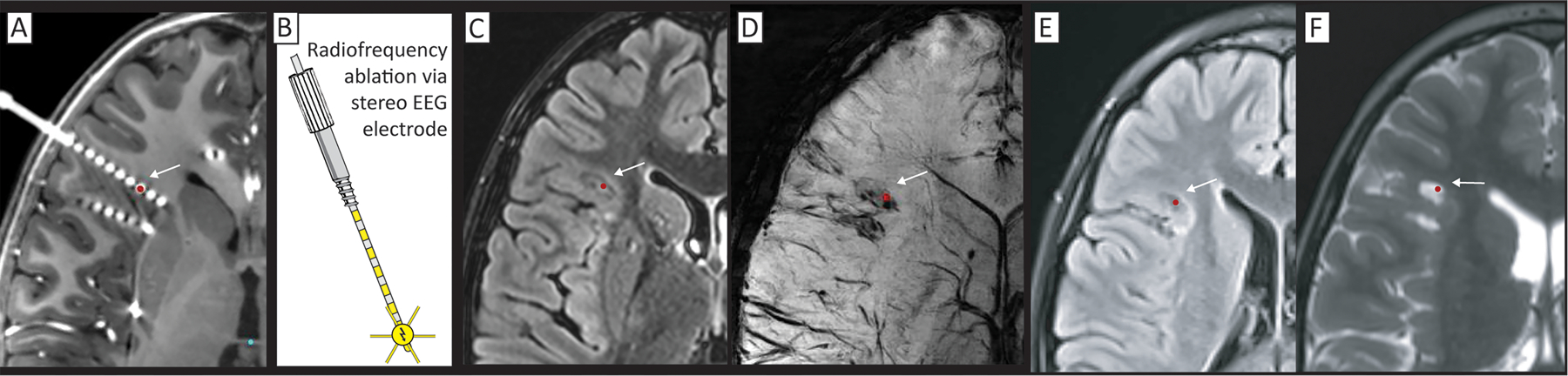
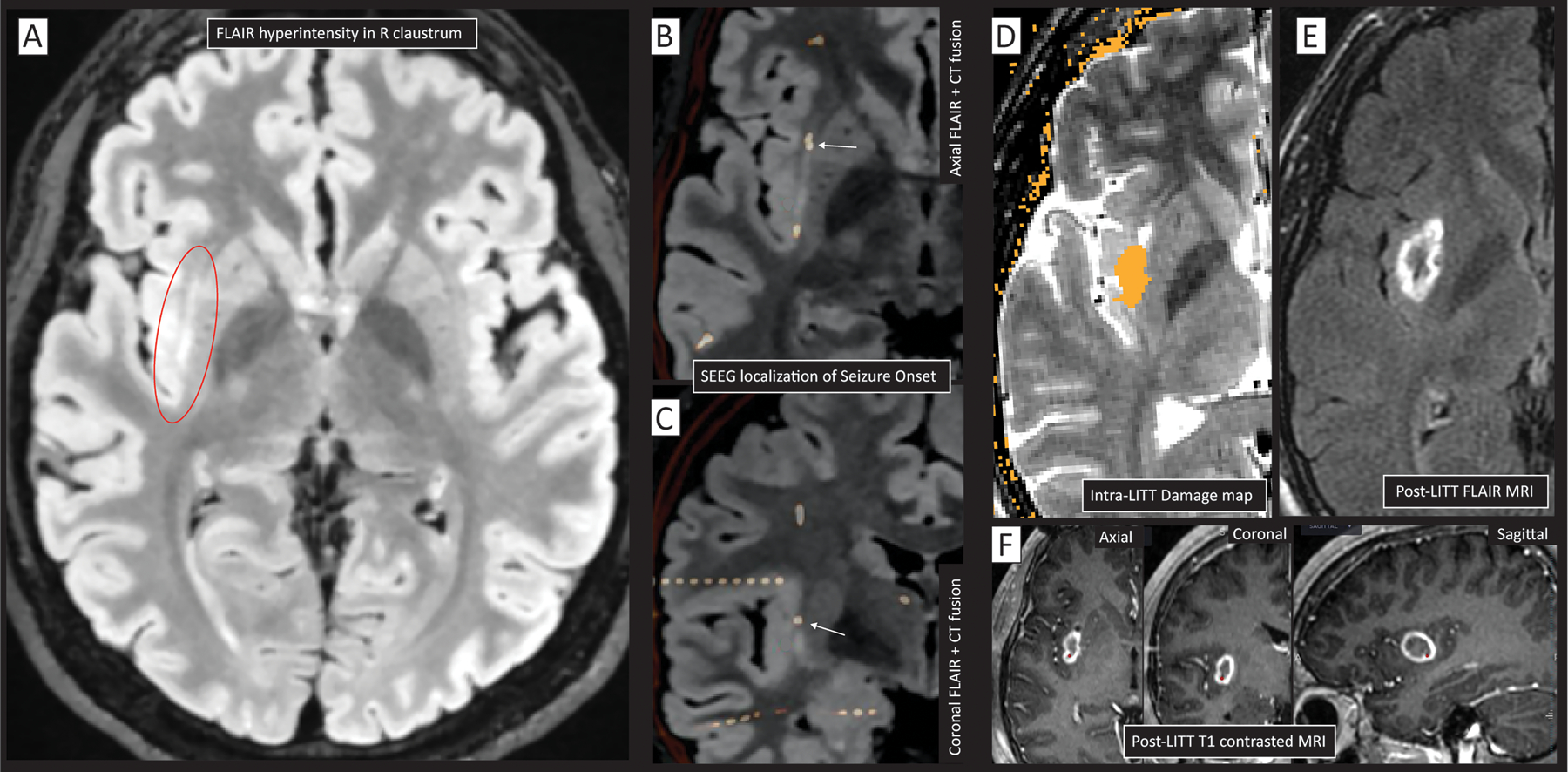
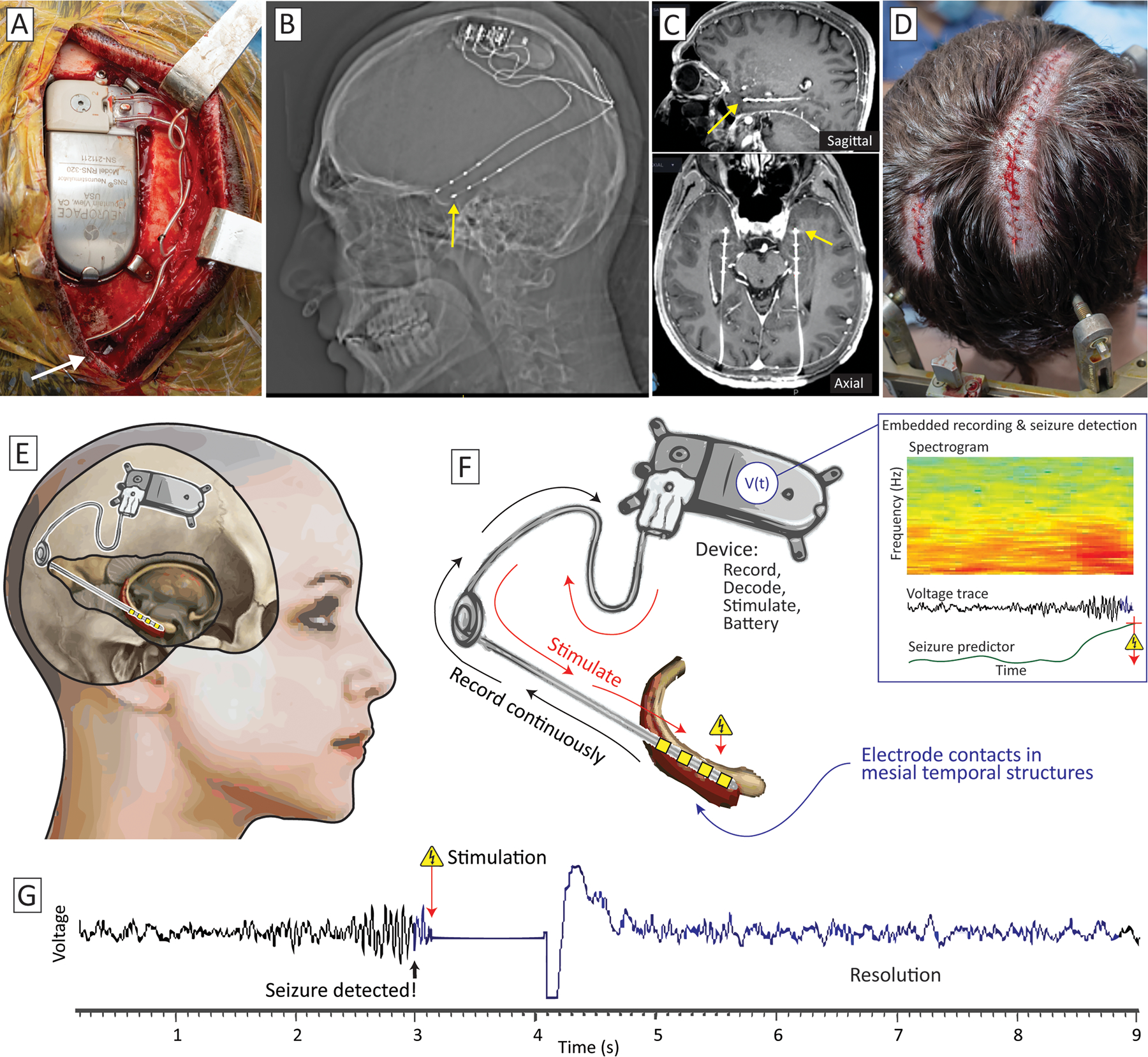
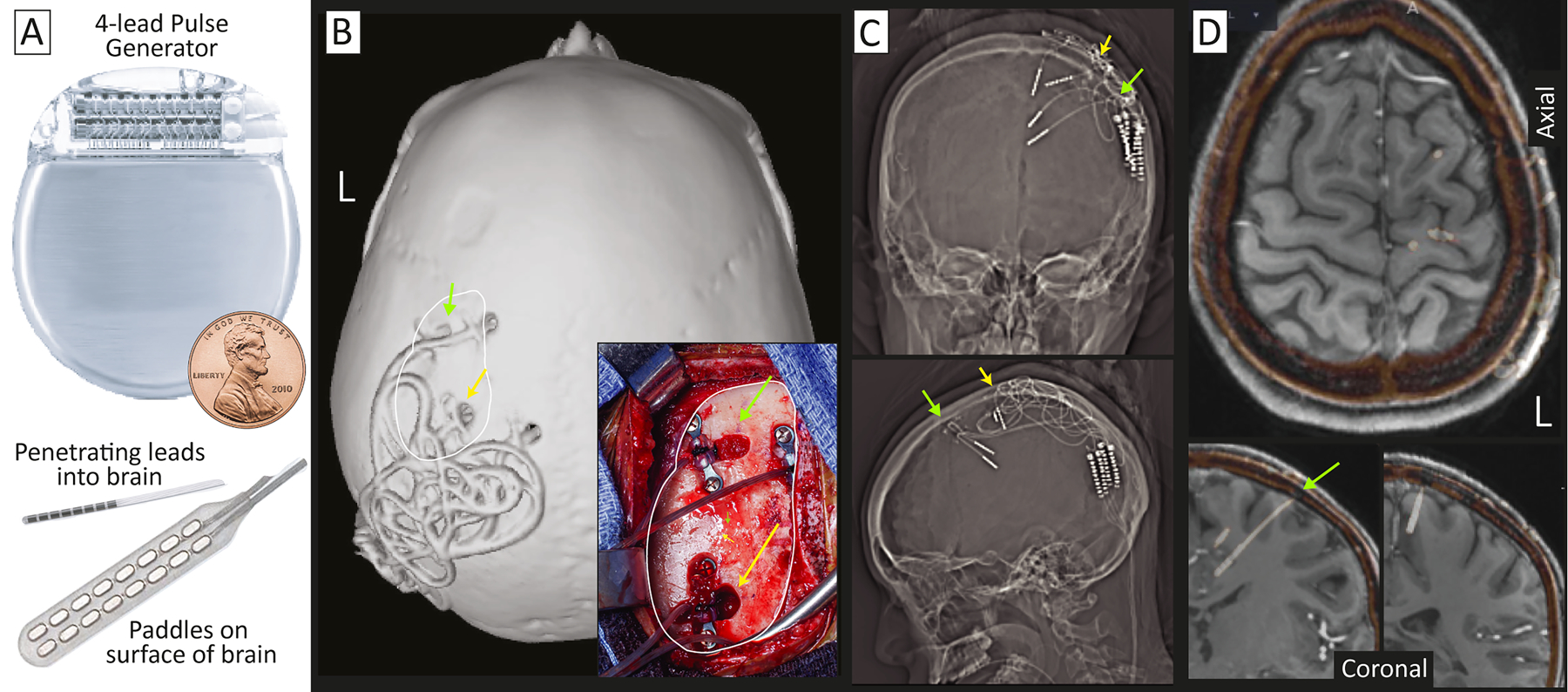
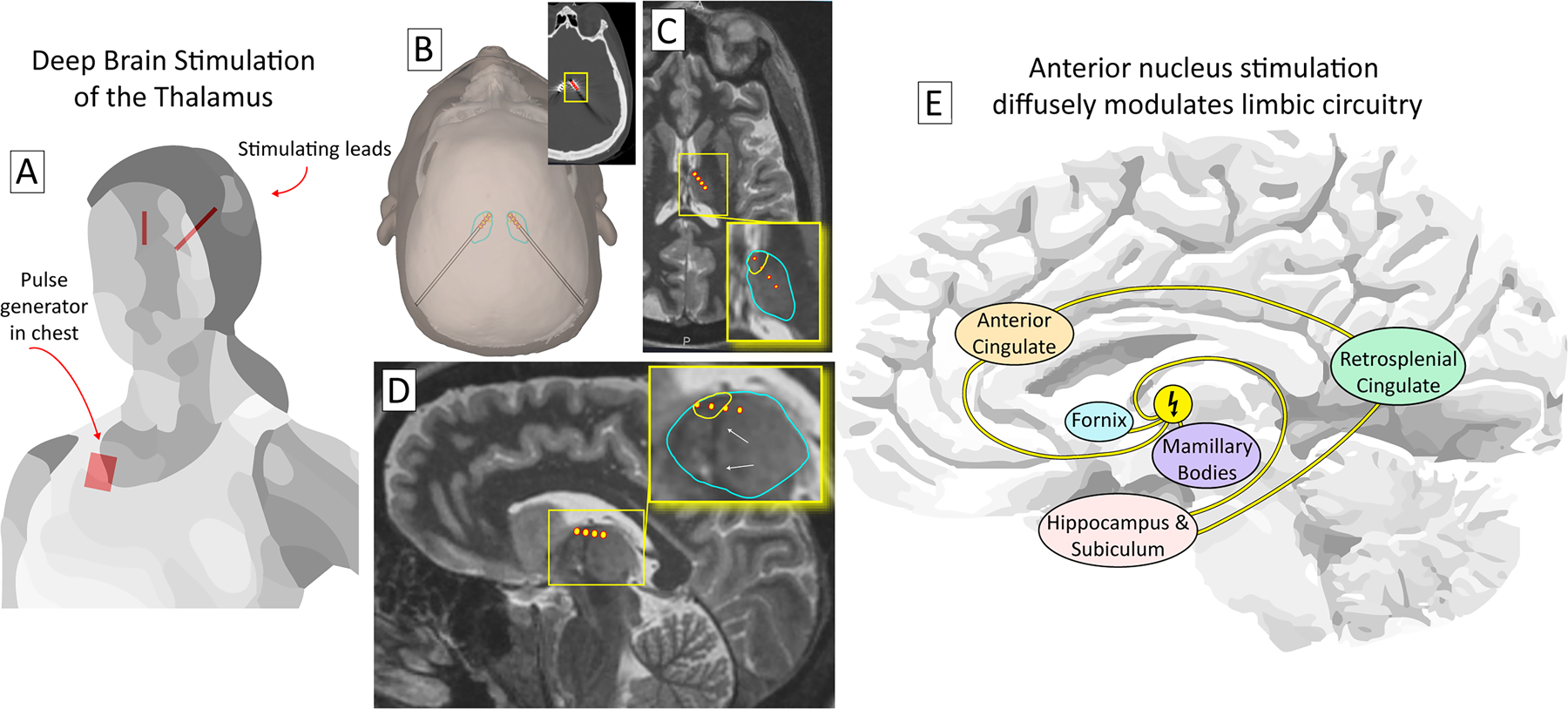
Surgery can cure or significantly improve both the frequency and the intensity of seizures in patients with medication-refractory epilepsy. The set of diagnostic and therapeutic interventions involved in the path from initial consultation to definitive surgery is complex and includes a multidisciplinary team of neurologists, neurosurgeons, neuroradiologists, and neuropsychologists, supported by a very large epilepsy-dedicated clinical architecture. In recent years, new practices and technologies have emerged that dramatically expand the scope of interventions performed. Stereoelectroencephalography has become widely adopted for seizure localization; stereotactic laser ablation has enabled more focal, less invasive, and less destructive interventions; and new brain stimulation devices have unlocked treatment of eloquent foci and multifocal onset etiologies. This article articulates and illustrates the full framework for how epilepsy patients are considered for surgical intervention, with particular attention given to stereotactic approaches.
Keywords: epilepsy; neurosurgery; stereotaxy.
© 2022 International League Against Epilepsy.
Figures
References
-
- Kwan P, Brodie MJ. Early identification of refractory epilepsy N Engl J Med 2000. Feb 3;342:314–319. - PubMed
-
- Callaghan BC, Anand K, Hesdorffer D, Hauser WA, French JA. Likelihood of seizure remission in an adult population with refractory epilepsy Ann Neurol 2007. Oct;62:382–389. - PubMed
-
- Luciano AL, Shorvon SD. Results of treatment changes in patients with apparently drug-resistant chronic epilepsy Ann Neurol 2007. Oct;62:375–381. - PubMed
-
- Kwan P, Schachter SC, Brodie MJ. Drug-resistant epilepsy N Engl J Med 2011. Sep 8;365:919–926. - PubMed
-
- Jobst BC, Cascino GD. Resective epilepsy surgery for drug-resistant focal epilepsy: a review JAMA 2015. Jan 20;313:285–293. - PubMed
