

A mid-level health manager intervention to promote uptake of isoniazid preventive therapy among people with HIV in Uganda: a cluster randomised trial
- PMID: 35908553
- PMCID: PMC9536151
- DOI: 10.1016/S2352-3018(22)00166-7
A mid-level health manager intervention to promote uptake of isoniazid preventive therapy among people with HIV in Uganda: a cluster randomised trial
Abstract
Background: Despite longstanding guidelines endorsing isoniazid preventive therapy (IPT) for people with HIV, uptake is low across sub-Saharan Africa. Mid-level health managers oversee IPT programmes nationally; interventions aimed at this group have not been tested. We aimed to establish whether providing structured leadership and management training and facilitating subregional collaboration and routine data feedback to mid-level managers could increase IPT initiation among people with HIV compared with standard practice.
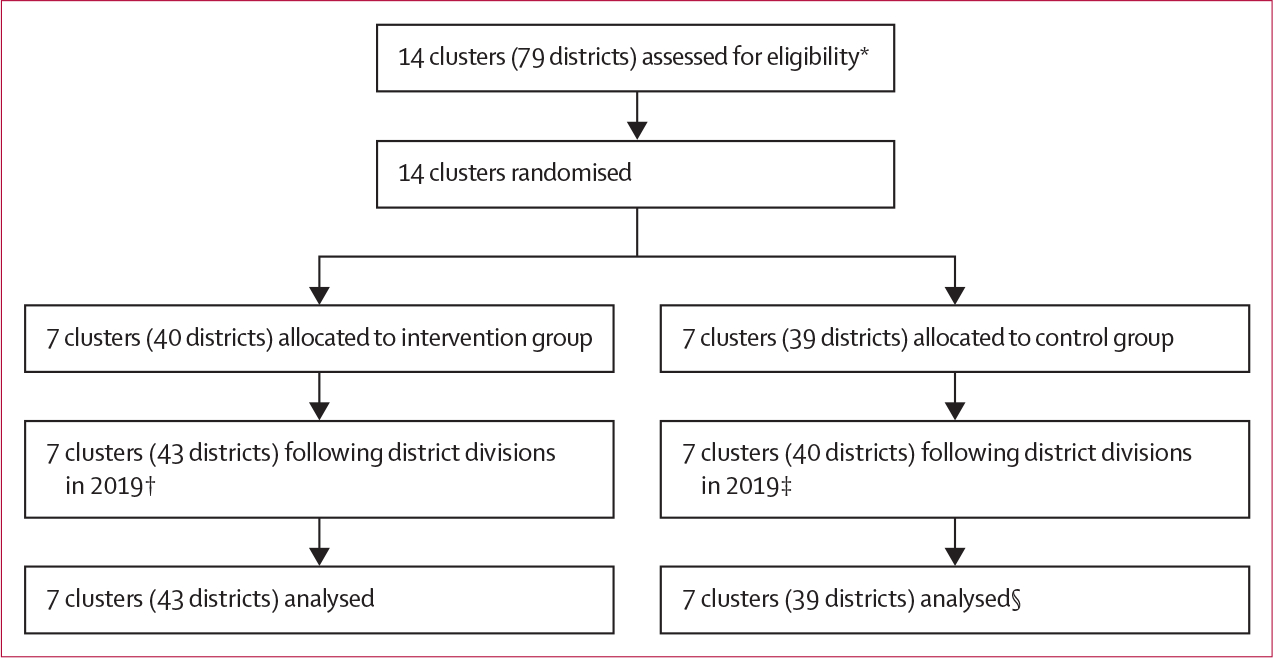
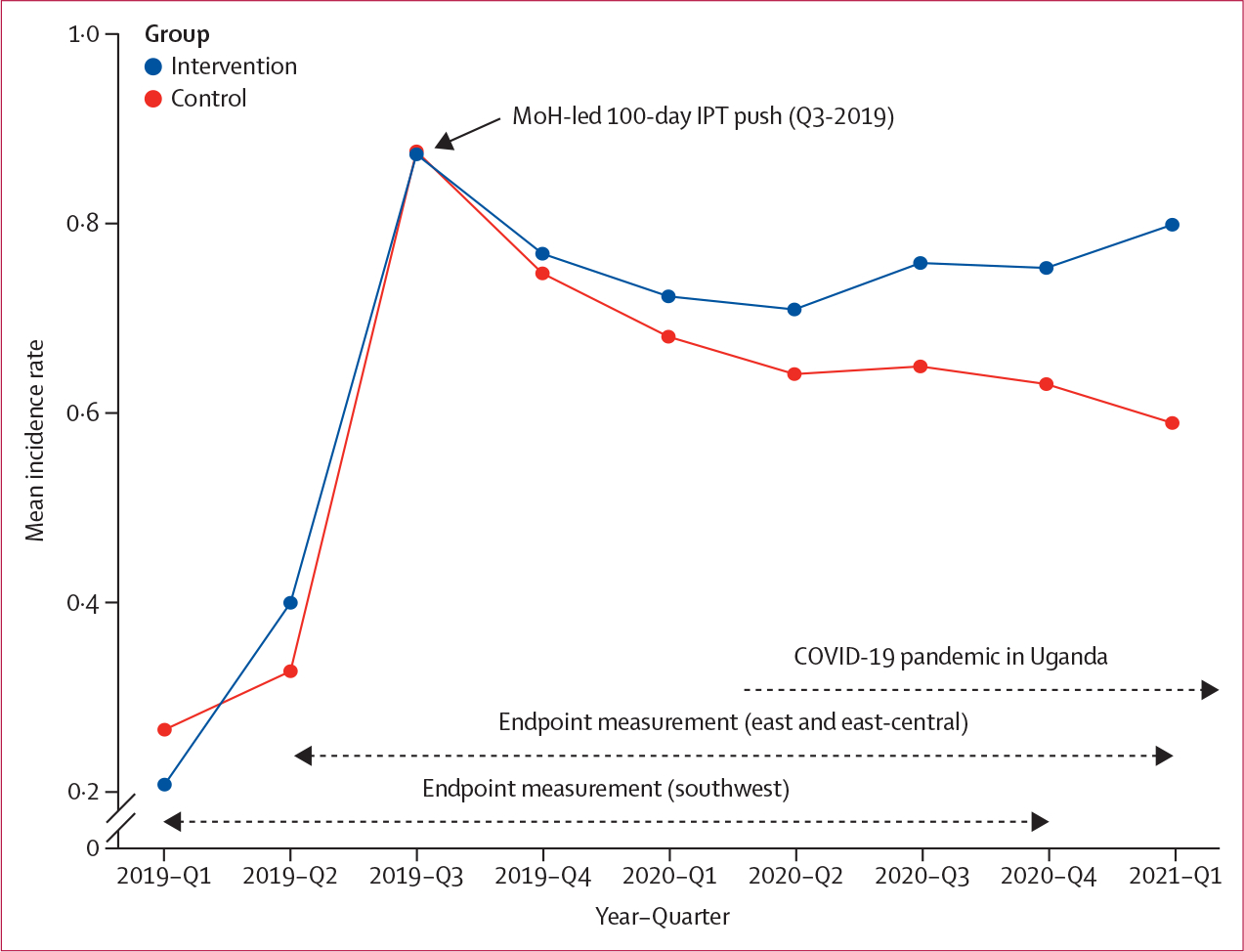
Methods: We conducted a cluster randomised trial in Uganda among district-level health managers. We randomly assigned clusters of between four and seven managers in a 1:1 ratio to intervention or control groups. Our intervention convened managers into mini-collaboratives facilitated by Ugandan experts in tuberculosis and HIV, and provided business leadership and management training, SMS platform access, and data feedback. The control was standard practice. Participants were not masked to trial group, but study statisticians were masked until trial completion. The primary outcome was IPT initiation rates among adults with HIV in facilities overseen by participants over a period of 2 years (2019-21). We conducted prespecified analyses that excluded the third quarter of 2019 (Q3-2019) to understand intervention effects independent of a national 100-day IPT push tied to a financial contingency during Q3-2019. This trial is registered with ClinicalTrials.gov (NCT03315962), and is ongoing.
Findings: Between Nov 15, 2017, and March 14, 2018, managers from 82 of 82 eligible districts (61% of Uganda's 135 districts) were enrolled and randomised: 43 districts to intervention, 39 to control. Intervention delivery took place between Dec 6, 2017, and Feb 2, 2022. Over 2 years, IPT initiation rates were 0·74 versus 0·65 starts per person-year in intervention versus control groups (incidence rate ratio [IRR] 1·14, 95% CI 0·88-1·46; p=0·16). Excluding Q3-2019, IPT initiation was higher in the intervention group versus the control group: 0·32 versus 0·25 starts per person-year (IRR 1·27, 95% CI 1·00-1·61; p=0·026).
Interpretation: Following an intervention targeting managers in more than 60% of Uganda's districts, IPT initiation rates were not significantly higher in intervention than control groups. After accounting for large increases in IPT from a 100-day push in both groups, the intervention led to significantly increased IPT rates, sustained after the push and during the COVID-19 pandemic. Our findings suggest that interventions centred on mid-level health managers can improve IPT implementation on a large, subnational scale, and merit further exploration to address key public health challenges for which strong evidence exists but implementation remains suboptimal.
Funding: National Institute of Allergy and Infectious Diseases.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Promoting tuberculosis preventive therapy in HIV.Lancet HIV. 2022 Sep;9(9):e596-e597. doi: 10.1016/S2352-3018(22)00197-7. Epub 2022 Jul 28. Lancet HIV. 2022. PMID: 35908552 No abstract available.
-
Young children still to treat, unfortunately.Lancet HIV. 2022 Sep;9(9):e600-e601. doi: 10.1016/S2352-3018(22)00199-0. Lancet HIV. 2022. PMID: 36055290 No abstract available.
References
-
- WHO. Global tuberculosis report 2020. Geneva: World Health Organization, 2020.
-
- Getahun H, Granich R, Sculier D, et al. Implementation of isoniazid preventive therapy for people living with HIV worldwide: barriers and solutions. AIDS 2010; 24 (suppl 5): S57–65. - PubMed
-
- WHO. Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource-constrained settings. Geneva: World Health Organization, 2011.
