

JNK pathway-associated phosphatase illustrates low expression and negative correlations with inflammation, disease activity, and T-helper 17 cells in inflammatory bowel disease children
- PMID: 35908771
- PMCID: PMC9459247
- DOI: 10.1002/jcla.24488
JNK pathway-associated phosphatase illustrates low expression and negative correlations with inflammation, disease activity, and T-helper 17 cells in inflammatory bowel disease children
Abstract
Background: C-Jun N-terminal kinase pathway-associated phosphatase (JKAP) modulates the T cell receptor and mitogen-activated protein kinase pathway-mediated autoimmunity, thus participating in the pathogenesis of autoimmune diseases. This study aimed to explore the clinical implication of JKAP in inflammatory bowel disease (IBD) children.
Methods: C-Jun N-terminal kinase pathway-associated phosphatase, tumor necrosis factor-α (TNF-α), interleukin-23, interferon-γ (T-helper 1 secreted cytokine), and interleukin-17A (T-helper 17 secreted cytokine) in serum samples from 140 IBD children (including 60 Crohn's disease (CD) children and 80 ulcerative colitis (UC) children) were detected by ELISA. Meanwhile, JKAP from serum samples of 10 healthy controls (HCs) was also detected by ELISA.
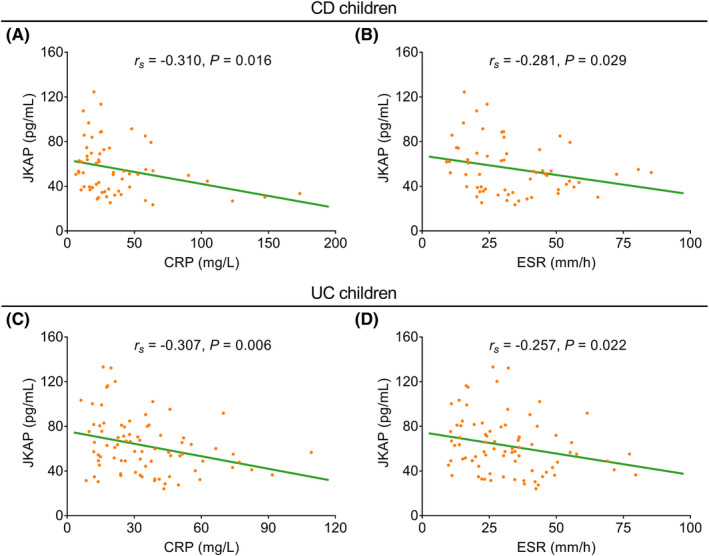
Results: C-Jun N-terminal kinase pathway-associated phosphatase was reduced in CD children (median (interquartile range (IQR)): 51.6 (36.8-69.5) pg/ml) and UC children (median (IQR): 57.5 (43.4-78.5) pg/ml) compared with HCs (median (IQR): 101.8 (70.0-143.2) pg/ml) (both p < 0.05). In CD children, JKAP was negatively correlated with C-reactive protein (CRP) (p = 0.016) and erythrocyte sedimentation rate (ESR) (p = 0.029); while in UC children, JKAP was also negatively correlated with CRP (p = 0.006) and ESR (p = 0.022). Regarding the correlation of JKAP with disease activity, it presented negative correlations with PCDAI (p = 0.001) and PUCAI (p = 0.002). Besides, JKAP was negatively related to TNF-α (both p < 0.05) but not interleukin-23 (both p>0.05) in CD and UC children. Additionally, JKAP was not correlated with interferon-γ in CD or UC children (both p>0.05), while negatively correlated with interleukin-17A in CD and UC children (both p < 0.05).
Conclusion: C-Jun N-terminal kinase pathway-associated phosphatase shows low expression and negative correlations with inflammation, disease activity, and T-helper 17 cells in IBD children.
Keywords: C-Jun N-terminal kinase pathway-associated phosphatase; T-helper 17; disease activity; inflammation; inflammatory bowel disease children.
© 2022 The Authors. Journal of Clinical Laboratory Analysis published by Wiley Periodicals LLC.
Conflict of interest statement
The authors have no relevant financial or non‐financial interests to disclose.
Figures





Similar articles
-
Circulating JNK pathway-associated phosphatase level correlates with decreased risk, activity, inflammation level and reduced clinical response to tumor necrosis factor-α inhibitor in Crohn disease patients.Medicine (Baltimore). 2019 Aug;98(33):e16622. doi: 10.1097/MD.0000000000016622. Medicine (Baltimore). 2019. PMID: 31415355 Free PMC article.
-
The correlation between Jun N-terminal kinase pathway-associated phosphatase and Th1 cell or Th17 cell in sepsis and their potential roles in clinical sepsis management.Ir J Med Sci. 2021 Aug;190(3):1173-1181. doi: 10.1007/s11845-020-02382-5. Epub 2020 Oct 20. Ir J Med Sci. 2021. PMID: 33083958 Free PMC article.
-
Serum inter-alpha-trypsin inhibitor heavy chain 4 in patients with inflammatory bowel disease: correlation with disease risk, inflammation, activity, and its variation after treatment.Ir J Med Sci. 2022 Oct;191(5):2105-2111. doi: 10.1007/s11845-021-02837-3. Epub 2021 Nov 29. Ir J Med Sci. 2022. PMID: 34843071
-
Study of tumor necrosis factor receptor in the inflammatory bowel disease.World J Gastroenterol. 2023 May 14;29(18):2733-2746. doi: 10.3748/wjg.v29.i18.2733. World J Gastroenterol. 2023. PMID: 37274062 Free PMC article. Review.
-
Differentiating ulcerative colitis from Crohn disease in children and young adults: report of a working group of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the Crohn's and Colitis Foundation of America.J Pediatr Gastroenterol Nutr. 2007 May;44(5):653-74. doi: 10.1097/MPG.0b013e31805563f3. J Pediatr Gastroenterol Nutr. 2007. PMID: 17460505
Cited by
-
Circulating JKAP levels may correlate with postpartum anxiety and depression through its interaction with T helper 17 cells.Braz J Med Biol Res. 2024 Oct 7;57:e13253. doi: 10.1590/1414-431X2024e13253. eCollection 2024. Braz J Med Biol Res. 2024. PMID: 39383378 Free PMC article.
-
BMSC exosomes deliver JKAP to restore Th17/Treg balance via AKT/ERK, alleviating rheumatoid arthritis.iScience. 2025 Jun 6;28(7):112832. doi: 10.1016/j.isci.2025.112832. eCollection 2025 Jul 18. iScience. 2025. PMID: 40687841 Free PMC article.
-
Enhanced diagnosis of pulmonary tuberculosis through nucleotide MALDI-TOF MS analysis of BALF: a retrospective clinical study.Sci Rep. 2024 Aug 8;14(1):18416. doi: 10.1038/s41598-024-66178-8. Sci Rep. 2024. PMID: 39117658 Free PMC article.
-
Thymoquinone Ameliorates Gut Epithelial Injury by Suppressing the JNK Signaling Pathway Based on Its Anti-Oxidant Property.Food Sci Nutr. 2025 Mar 24;13(4):e70113. doi: 10.1002/fsn3.70113. eCollection 2025 Apr. Food Sci Nutr. 2025. PMID: 40129997 Free PMC article.
References
-
- Rubalcava NS, Gadepalli SK. Inflammatory bowel disease in children and adolescents. Adv Pediatr. 2021;68:121‐142. - PubMed
-
- Flynn S, Eisenstein S. Inflammatory bowel disease presentation and diagnosis. Surg Clin North Am. 2019;99(6):1051‐1062. - PubMed
-
- Fuller MK. Pediatric inflammatory bowel disease: special considerations. Surg Clin North Am. 2019;99(6):1177‐1183. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
