

Nomogram for predicting rebleeding after initial endoscopic epinephrine injection monotherapy hemostasis in patients with peptic ulcer bleeding: a retrospective cohort study
- PMID: 35909111
- PMCID: PMC9341049
- DOI: 10.1186/s12876-022-02448-x
Nomogram for predicting rebleeding after initial endoscopic epinephrine injection monotherapy hemostasis in patients with peptic ulcer bleeding: a retrospective cohort study
Abstract
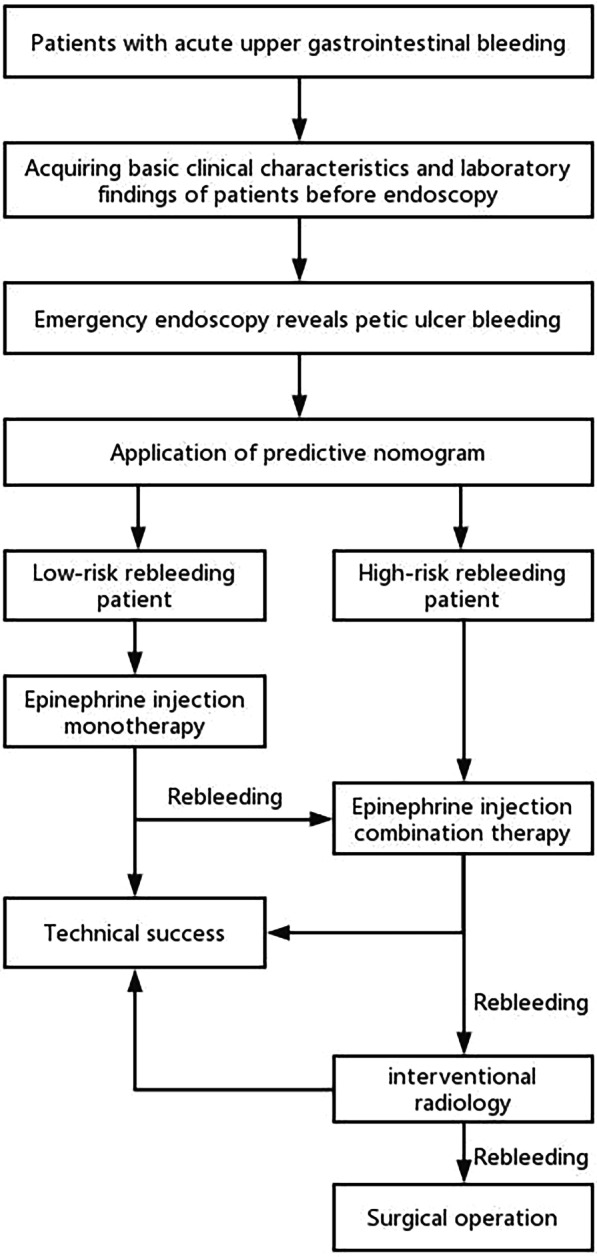
Background: Although the current guidelines recommend endoscopic combination therapy, endoscopic epinephrine injection (EI) monotherapy is still a simple, common and effective modality for treating peptic ulcer bleeding (PUB). However, the rebleeding risk after EI monotherapy is still high, and identifying rebleeding patients after EI monotherapy is unclear, which is highly important in clinical practice. This study aimed to identify risk factors and constructed a predictive nomogram related to rebleeding after EI monotherapy.
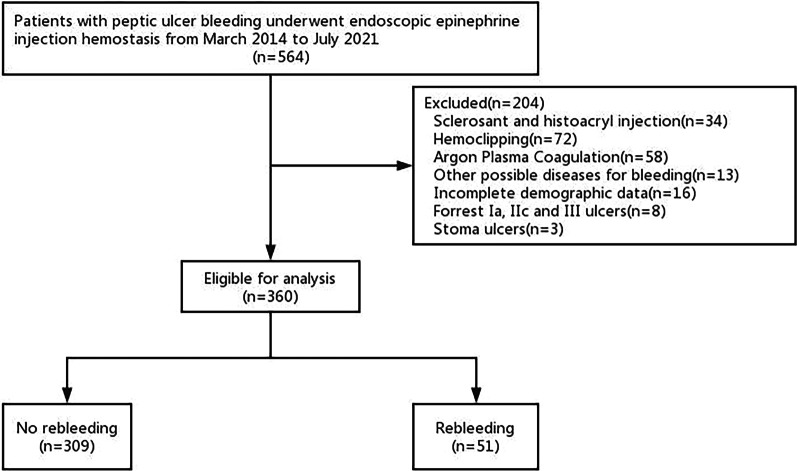
Methods: We consecutively and retrospectively analyzed 360 PUB patients who underwent EI monotherapy between March 2014 and July 2021 in our center. Then we identified independent risk factors associated with rebleeding after initial endoscopic EI monotherapy by multivariate logistic regression. A predictive nomogram was developed and validated based on the above predictors.
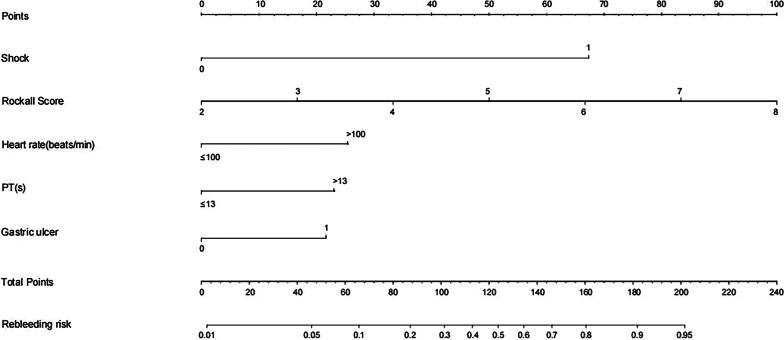
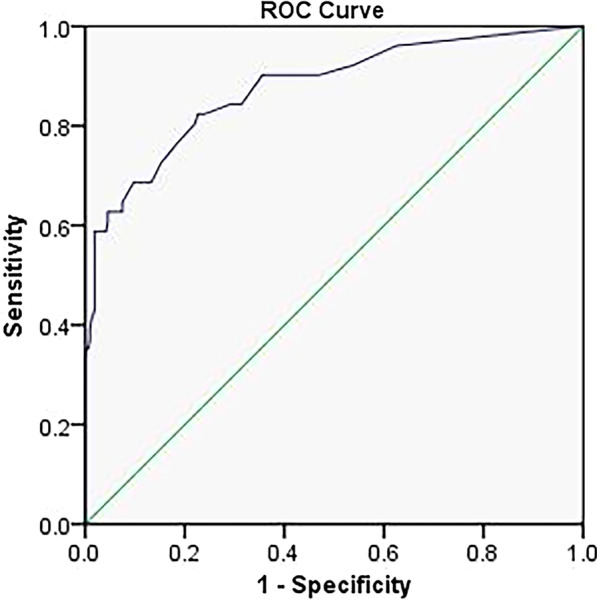
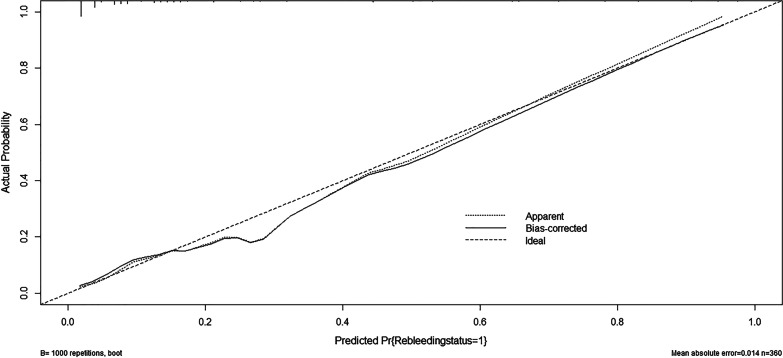
Results: Among all PUB patients enrolled, 51 (14.2%) had recurrent hemorrhage within 30 days after endoscopic EI monotherapy. After multivariate logistic regression, shock [odds ratio (OR) = 12.691, 95% confidence interval (CI) 5.129-31.399, p < 0.001], Rockall score (OR = 1.877, 95% CI 1.250-2.820, p = 0.002), tachycardia (heart rate > 100 beats/min) (OR = 2.610, 95% CI 1.098-6.203, p = 0.030), prolonged prothrombin time (PT > 13 s) (OR = 2.387, 95% CI 1.019-5.588, p = 0.045) and gastric ulcer (OR = 2.258, 95% CI 1.003-5.084, p = 0.049) were associated with an increased risk of rebleeding after an initial EI monotherapy treatment. A nomogram incorporating these independent high-risk factors showed good discrimination, with an area under the receiver operating characteristic curve (AUROC) of 0.876 (95% CI 0.817-0.934) (p < 0.001).
Conclusions: We developed a predictive nomogram of rebleeding after EI monotherapy, which had excellent prediction accuracy. This predictive nomogram can be conveniently used to identify low-risk rebleeding patients after EI monotherapy, allowing for decision-making in a clinical setting.
Keywords: Epinephrine injection monotherapy; Nomogram; Peptic ulcer bleeding; Rebleeding; Risk factors.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Predictors of rebleeding after initial hemostasis with epinephrine injection in high-risk ulcers.World J Gastroenterol. 2010 Nov 21;16(43):5490-5. doi: 10.3748/wjg.v16.i43.5490. World J Gastroenterol. 2010. PMID: 21086569 Free PMC article.
-
Development and validation of a model to predict rebleeding within three days after endoscopic hemostasis for high-risk peptic ulcer bleeding.BMC Gastroenterol. 2022 Feb 14;22(1):64. doi: 10.1186/s12876-022-02145-9. BMC Gastroenterol. 2022. PMID: 35164682 Free PMC article. Clinical Trial.
-
Epinephrine injection monotherapy shows similar hemostatic efficacy to epinephrine injection combined therapy in high-risk patients (Forrest Ib) with bleeding ulcers.Surg Endosc. 2023 Sep;37(9):6954-6963. doi: 10.1007/s00464-023-10152-4. Epub 2023 Jun 19. Surg Endosc. 2023. PMID: 37336844 Free PMC article.
-
Endoscopic Versus Conservative Therapy for Bleeding Peptic Ulcer with Adherent Clot: A Comprehensive Systematic Review and Meta-Analysis.Dig Dis Sci. 2023 Oct;68(10):3921-3934. doi: 10.1007/s10620-023-08078-x. Epub 2023 Aug 27. Dig Dis Sci. 2023. PMID: 37634184
-
Systematic Review and Meta-Analysis of Prophylactic Transarterial Embolization for High-Risk Bleeding Peptic Ulcer Disease.J Vasc Interv Radiol. 2021 Apr;32(4):576-584.e5. doi: 10.1016/j.jvir.2020.12.005. Epub 2021 Jan 29. J Vasc Interv Radiol. 2021. PMID: 33526343
Cited by
-
Risk factors and prediction model for rebleeding in grade IIb peptic ulcer patients after endoscopy.Am J Transl Res. 2025 Mar 15;17(3):2124-2134. doi: 10.62347/CJAZ6726. eCollection 2025. Am J Transl Res. 2025. PMID: 40225981 Free PMC article.
References
MeSH terms
Substances
Grants and funding
- 20212BDH81019/Science and Technology Department of Jiangxi Province
- 20212BDH81019/Science and Technology Department of Jiangxi Province
- 20212BDH81019/Science and Technology Department of Jiangxi Province
- 20212BDH81019/Science and Technology Department of Jiangxi Province
- 20212BDH81019/Science and Technology Department of Jiangxi Province
LinkOut - more resources
Full Text Sources
