

Influence of temperature management at 33 °C versus normothermia on survival in patients with vasopressor support after out-of-hospital cardiac arrest: a post hoc analysis of the TTM-2 trial
- PMID: 35909163
- PMCID: PMC9339193
- DOI: 10.1186/s13054-022-04107-9
Influence of temperature management at 33 °C versus normothermia on survival in patients with vasopressor support after out-of-hospital cardiac arrest: a post hoc analysis of the TTM-2 trial
Abstract
Background: Targeted temperature management at 33 °C (TTM33) has been employed in effort to mitigate brain injury in unconscious survivors of out-of-hospital cardiac arrest (OHCA). Current guidelines recommend prevention of fever, not excluding TTM33. The main objective of this study was to investigate if TTM33 is associated with mortality in patients with vasopressor support on admission after OHCA.
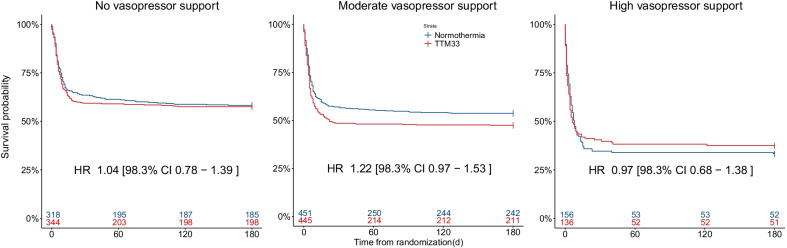
Methods: We performed a post hoc analysis of patients included in the TTM-2 trial, an international, multicenter trial, investigating outcomes in unconscious adult OHCA patients randomized to TTM33 versus normothermia. Patients were grouped according to level of circulatory support on admission: (1) no-vasopressor support, mean arterial blood pressure (MAP) ≥ 70 mmHg; (2) moderate-vasopressor support MAP < 70 mmHg or any dose of dopamine/dobutamine or noradrenaline/adrenaline dose ≤ 0.25 µg/kg/min; and (3) high-vasopressor support, noradrenaline/adrenaline dose > 0.25 µg/kg/min. Hazard ratios with TTM33 were calculated for all-cause 180-day mortality in these groups.
Results: The TTM-2 trial enrolled 1900 patients. Data on primary outcome were available for 1850 patients, with 662, 896, and 292 patients in the, no-, moderate-, or high-vasopressor support groups, respectively. Hazard ratio for 180-day mortality was 1.04 [98.3% CI 0.78-1.39] in the no-, 1.22 [98.3% CI 0.97-1.53] in the moderate-, and 0.97 [98.3% CI 0.68-1.38] in the high-vasopressor support groups with regard to TTM33. Results were consistent in an imputed, adjusted sensitivity analysis.
Conclusions: In this exploratory analysis, temperature control at 33 °C after OHCA, compared to normothermia, was not associated with higher incidence of death in patients stratified according to vasopressor support on admission. Trial registration Clinical trials identifier NCT02908308 , registered September 20, 2016.
Keywords: Cardiac arrest; Heart arrest; Hypothermia induced; Mortality; Shock; Sudden.
© 2022. The Author(s).
Conflict of interest statement
JD: No financial or non-financial competing interests. MA: No financial or non-financial competing interests. AC: Received fees for lectures from Bard. MC: No financial or non-financial competing interests. JD: No financial or non-financial competing interests. HF: TEQCool (Lund, Sweden) Academic advisor. MH: No financial or non-financial competing interests. ZH: No financial or non-financial competing interests. JCJ: No financial or non-financial competing interests. HL: No financial or non-financial competing interests. FT: No financial or non-financial competing interests. MT: No financial competing interests, co-applicant on several NIHR cardiac arrest trials but not in the field of temperature management. SU: No financial or non-financial competing interests. MPW: No financial or non-financial competing interests. NN: No financial or non-financial competing interests.
Figures
Similar articles
-
Hemodynamics and vasopressor support during targeted temperature management at 33°C Versus 36°C after out-of-hospital cardiac arrest: a post hoc study of the target temperature management trial*.Crit Care Med. 2015 Feb;43(2):318-27. doi: 10.1097/CCM.0000000000000691. Crit Care Med. 2015. PMID: 25365723 Clinical Trial.
-
Hypothermia vs Normothermia in Patients With Cardiac Arrest and Nonshockable Rhythm: A Meta-Analysis.JAMA Neurol. 2024 Feb 1;81(2):126-133. doi: 10.1001/jamaneurol.2023.4820. JAMA Neurol. 2024. PMID: 38109117 Free PMC article.
-
Level of systemic inflammation and endothelial injury is associated with cardiovascular dysfunction and vasopressor support in post-cardiac arrest patients.Resuscitation. 2017 Dec;121:179-186. doi: 10.1016/j.resuscitation.2017.09.019. Epub 2017 Sep 23. Resuscitation. 2017. PMID: 28947390 Clinical Trial.
-
Epinephrine for Out-of-Hospital Cardiac Arrest: An Updated Systematic Review and Meta-Analysis.Crit Care Med. 2020 Feb;48(2):225-229. doi: 10.1097/CCM.0000000000004130. Crit Care Med. 2020. PMID: 31939791
-
Hypothermia versus normothermia after out-of-hospital cardiac arrest: A systematic review and meta-analysis of randomized controlled trials.Ann Med Surg (Lond). 2022 Jan 29;74:103327. doi: 10.1016/j.amsu.2022.103327. eCollection 2022 Feb. Ann Med Surg (Lond). 2022. PMID: 35145684 Free PMC article. Review.
Cited by
-
Outcomes of mild-to-moderate postresuscitation shock after non-shockable cardiac arrest and association with temperature management: a post hoc analysis of HYPERION trial data.Ann Intensive Care. 2022 Oct 17;12(1):96. doi: 10.1186/s13613-022-01071-z. Ann Intensive Care. 2022. PMID: 36251223 Free PMC article.
-
Development and validation of prediction models for death within 6 months after cardiac arrest.Front Cardiovasc Med. 2024 Nov 28;11:1469801. doi: 10.3389/fcvm.2024.1469801. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39669409 Free PMC article.
-
Ten rules for optimizing ventilatory settings and targets in post-cardiac arrest patients.Crit Care. 2022 Dec 17;26(1):390. doi: 10.1186/s13054-022-04268-7. Crit Care. 2022. PMID: 36527126 Free PMC article. Review.
-
Trend of Outcome Metrics in Recent Out-of-Hospital-Cardiac-Arrest Research: A Narrative Review of Clinical Trials.J Clin Med. 2023 Nov 20;12(22):7196. doi: 10.3390/jcm12227196. J Clin Med. 2023. PMID: 38002808 Free PMC article. Review.
-
Comparison of hypothermic and normothermic targeted temperature management in out-of-hospital cardiac arrest patients with acute coronary syndrome: a nationwide retrospective study.Crit Care. 2025 Jan 6;29(1):6. doi: 10.1186/s13054-024-05235-0. Crit Care. 2025. PMID: 39762968 Free PMC article.
