

Riociguat in pulmonary hypertension and heart failure with preserved ejection fraction: the haemoDYNAMIC trial
- PMID: 35909264
- PMCID: PMC9492239
- DOI: 10.1093/eurheartj/ehac389
Riociguat in pulmonary hypertension and heart failure with preserved ejection fraction: the haemoDYNAMIC trial
Abstract
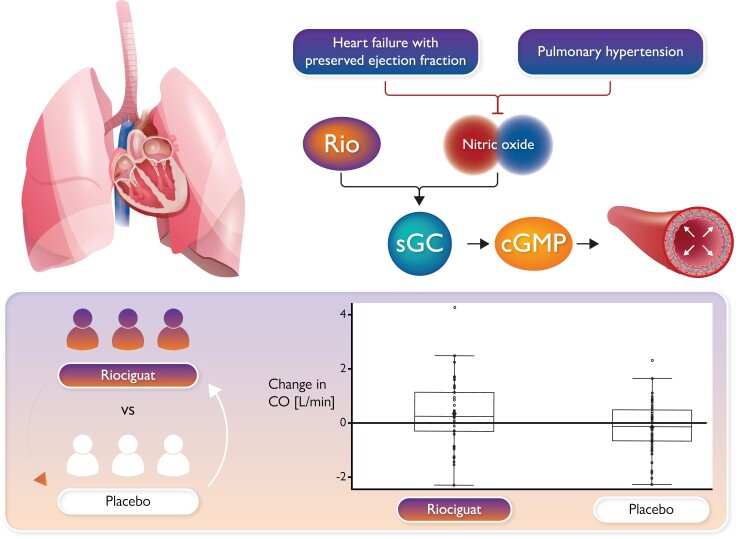
Aims: The presence of pulmonary hypertension (PH) severely aggravates the clinical course of heart failure with preserved ejection fraction (HFpEF). To date, neither established heart failure therapies nor pulmonary vasodilators proved beneficial. This study investigated the efficacy of chronic treatment with the oral soluble guanylate cyclase stimulator riociguat in patients with PH-HFpEF.
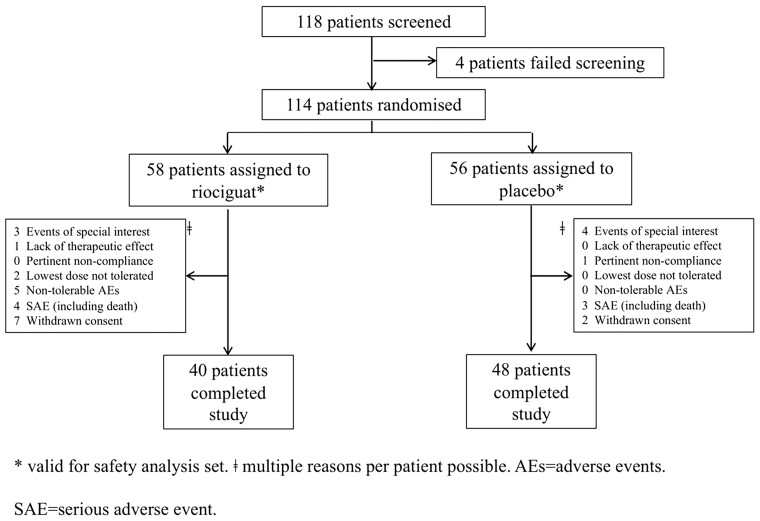
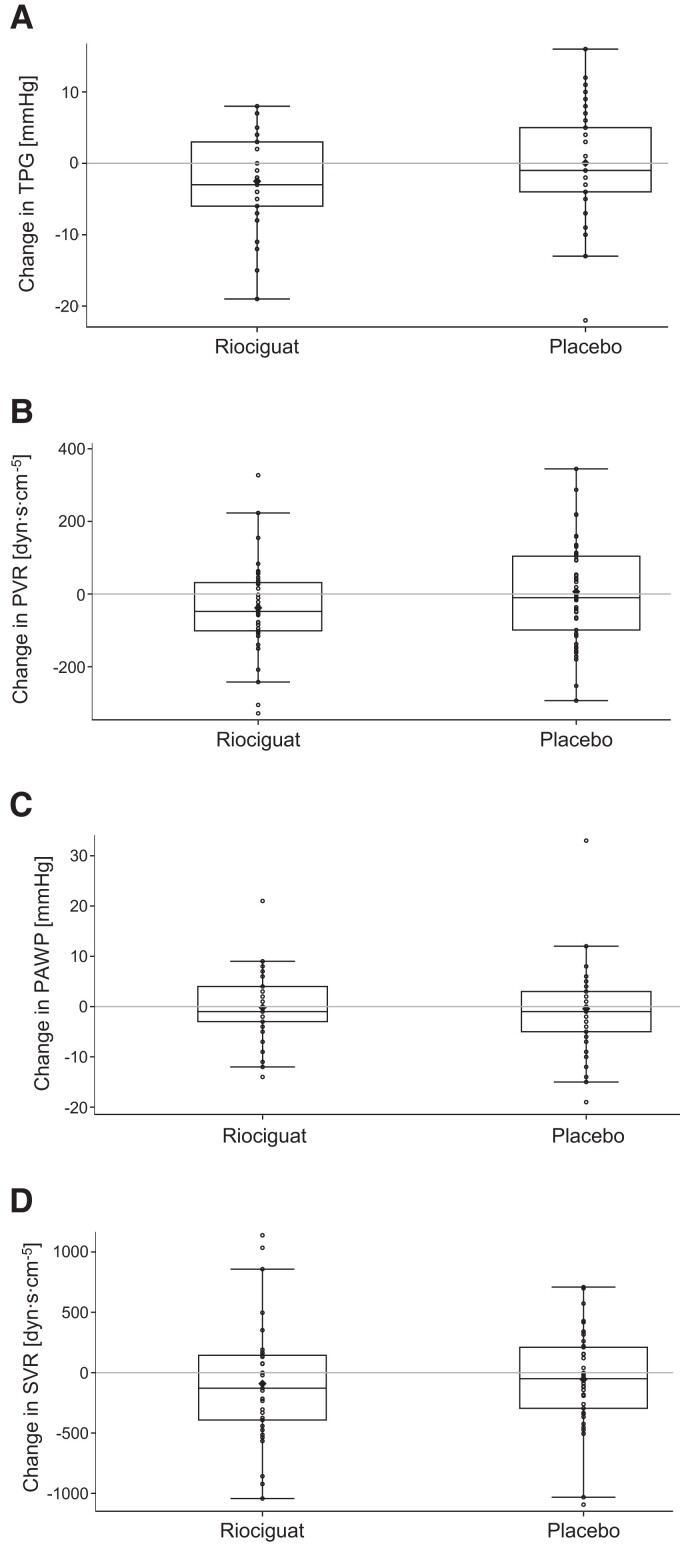
Methods and results: The phase IIb, randomized, double-blind, placebo-controlled, parallel-group, multicentre DYNAMIC trial assessed riociguat in PH-HFpEF. Patients were recruited at five hospitals across Austria and Germany. Key eligibility criteria were mean pulmonary artery pressure ≥25 mmHg, pulmonary arterial wedge pressure >15 mmHg, and left ventricular ejection fraction ≥50%. Patients were randomized to oral treatment with riociguat or placebo (1:1). Patients started at 0.5 mg three times daily (TID) and were up-titrated to 1.5 mg TID. The primary efficacy endpoint was change from baseline to week 26 in cardiac output (CO) at rest, measured by right heart catheterization. Primary efficacy analyses were performed on the full analysis set. Fifty-eight patients received riociguat and 56 patients placebo. After 26 weeks, CO increased by 0.37 ± 1.263 L/min in the riociguat group and decreased by -0.11 ± 0.921 L/min in the placebo group (least-squares mean difference: 0.54 L/min, 95% confidence interval 0.112, 0.971; P = 0.0142). Five patients dropped out due to riociguat-related adverse events but no riociguat-related serious adverse event or death occurred.
Conclusion: The vasodilator riociguat improved haemodynamics in PH-HFpEF. Riociguat was safe in most patients but led to more dropouts as compared to placebo and did not change clinical symptoms within the study period.
Keywords: Heart failure with preserved ejection fraction; Pulmonary hypertension; Randomized controlled trial; Riociguat; Soluble guanylate cyclase stimulation.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Conflict of interest statement
Conflict of interest: E.G. received grants/contracts from Bayer, MSD, United Therapeutics and OMT; consulting fees from Bayer, GlaxoSmithKline, Janssen, MSD, Merck, Sharp & Dohme, and United Therapeutics; payments/honoraria from Bayer, Janssen and MSD; support for attending meetings and/or travel from Bayer, GlaxoSmithKline, Janssen, MSD, Merck, Sharp & Dohme, and United Therapeutics. E.G. participated on data monitoring/advisory boards for Janssen, United Therapeutics, and Acceleron. I.P. has received honoraria for lectures from Orion, AOP Orphan and Amomed. D.B. received financial support for the present manuscript in form of an unrestricted research grant by Bayer (all payments were made to the Medical University of Vienna); research grants by Pfizer, Alnylam, Ionis, SOBI, Novartis, Sanofi (all payments were made to the Medical University of Vienna); and payments/honoraria from Bayer AG, Pfizer, Alnylam, Ionis, SOBI, Novartis, Sanofi, Astra Zeneca, Boehringer Ingelheim, Zoll, Janssen, AOP Orphan, and MSD. All other authors declare that there is no conflict of interest.
Figures

Comment in
-
Targeting pulmonary hypertension in patients with heart failure and preserved ejection fraction: rather static than DYNAMIC development?Eur Heart J. 2022 Sep 21;43(36):3414-3416. doi: 10.1093/eurheartj/ehac387. Eur Heart J. 2022. PMID: 35909260 No abstract available.
References
-
- Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol 2017;14:591–602. - PubMed
-
- Guazzi M, Naeije R. Pulmonary hypertension in heart failure: pathophysiology, pathobiology, and emerging clinical perspectives. J Am Coll Cardiol 2017;69:1718–1734. - PubMed
-
- Hoeper MM, Carolyn SP, Lam CSP, Vachiery JL, Bauersachs J, Gerges C, et al. Pulmonary hypertension in heart failure with preserved ejection fraction: a plea for proper phenotyping and further research. Eur Heart J 2017;38:2869–873. - PubMed
-
- Borlaug BA. Evaluation and management of heart failure with preserved ejection fraction. Nat Rev Cardiol 2020;17:559–573. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
