

An Ovarian Large-Cell Neuroendocrine Carcinoma Accompanied by Clear Cell Carcinoma with Specific High Level of AFP: Case Report and Review of the Literature
- PMID: 35909650
- PMCID: PMC9326035
- DOI: 10.2147/CMAR.S366771
An Ovarian Large-Cell Neuroendocrine Carcinoma Accompanied by Clear Cell Carcinoma with Specific High Level of AFP: Case Report and Review of the Literature
Abstract
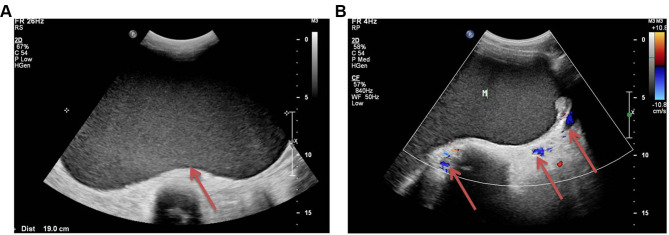
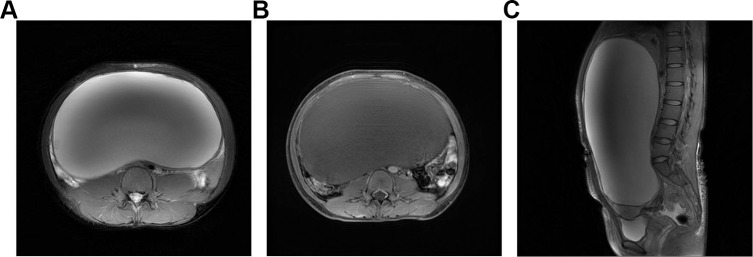
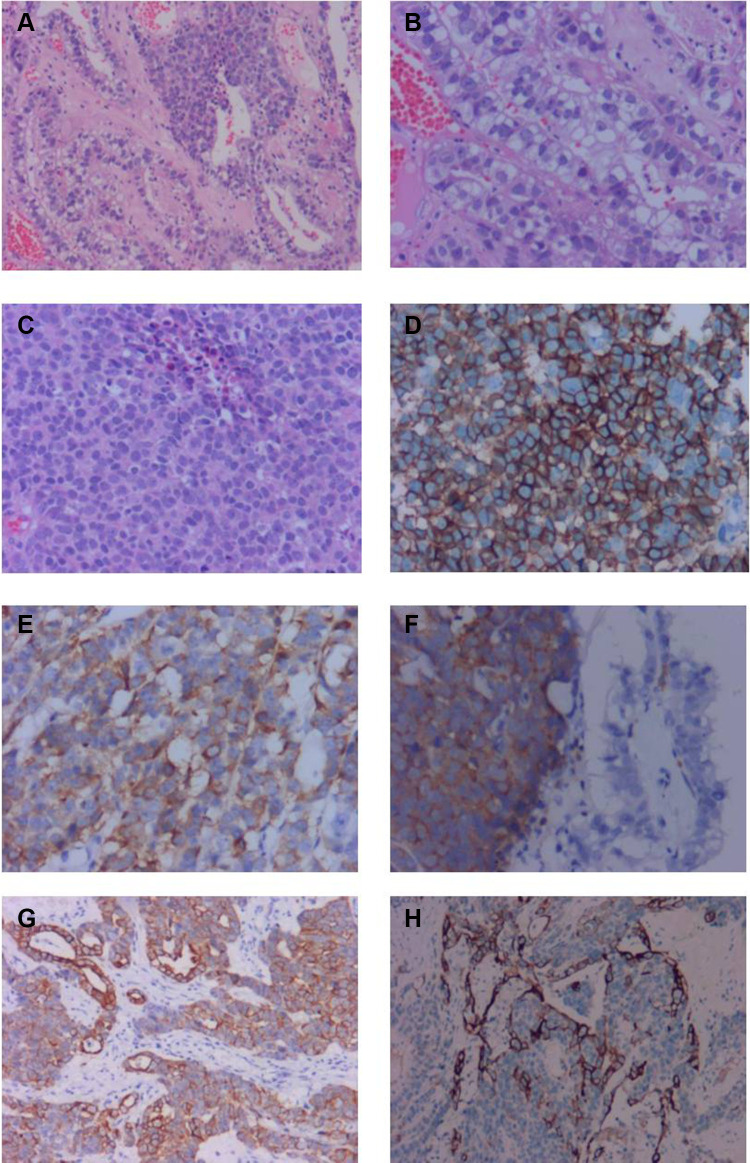
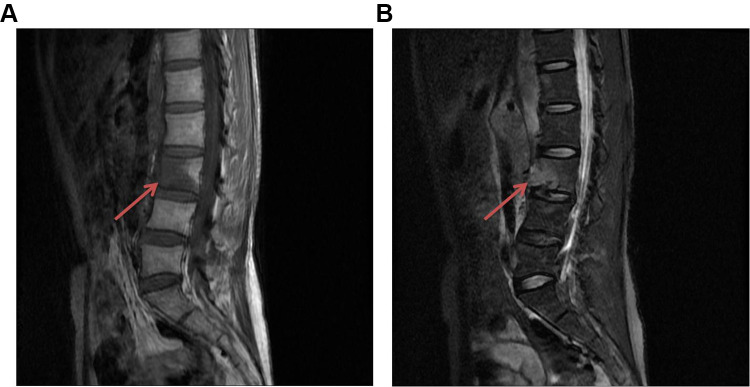
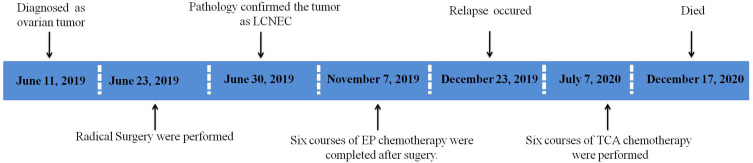
Large cell neuroendocrine carcinoma (LCNEC) is a rare histological subtype of ovarian cancer. A few cases have been reported in the literature with extreme invasiveness and a poor prognosis. However, there still have not been accepted criteria for diagnosis and treatment of LCNEC. Here we report an unmarried 37 year-old woman who was diagnosed with LCNEC associated with clear cell carcinoma and the tumor index was manifested with a specific increase of AFP. The case received six courses of etoposide and carboplatin chemotherapy as an adjuvant therapy after primary curative surgery. However, she relapsed within 6 months after surgery and metastasized rapidly to distant organs despite combined chemotherapy of paclitaxel, cisplatin, and bevacizumab, and died 18 months after primary surgery. This is the first reported case of LCNEC manifested with a specific increase of AFP and characteristically metastasized to the spine as recurrence. Reviewing our case as well as previously reported cases, LCNEC present with aggressive malignancy and vulnerable to distant metastasis through a hematogenous approach, we conjectured that adding Bevacizumab in primary chemotherapy may be beneficial to extend disease-free survival. But so far there is no recommendation of this regimen for treatment of LCNEC in current guidelines. Further research is needed to confirm this view so as to find the best treatment of LCNEC and improve the prognosis of these patients.
Keywords: large cell neuroendocrine carcinoma; ovarian tumors.
© 2022 Qiu et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest in relation to this work.
Figures
References
-
- Hirasawa T. Ovarian neuroendocrine carcinoma associated with mucinous carcinoma and teratoma. Nihon Rinsho. 2004;62(5):973–978. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
