

Prevalence of a History of Metabolic or Hypertensive Pregnancy Disorder in Patients With Myocardial Infarction and Non-obstructive Coronary Arteries: An Observational Cohort Study
- PMID: 35911523
- PMCID: PMC9334660
- DOI: 10.3389/fcvm.2022.932799
Prevalence of a History of Metabolic or Hypertensive Pregnancy Disorder in Patients With Myocardial Infarction and Non-obstructive Coronary Arteries: An Observational Cohort Study
Abstract
Introduction: Myocardial infarction with non-obstructive coronary arteries (MINOCA) predominantly affects younger females. Women with a history of gestational hypertension (GH), preeclampsia (PE), and gestational diabetes mellitus (GDM) are subjected to an elevated lifetime risk of cardiovascular disease. However, data on the potential association between these obstetric complications and MINOCA is lacking. Therefore, the current study aimed to provide insight in the prevalence of metabolic and hypertensive pregnancy disorders (MHPD) in MINOCA patients and their clinical characteristics.
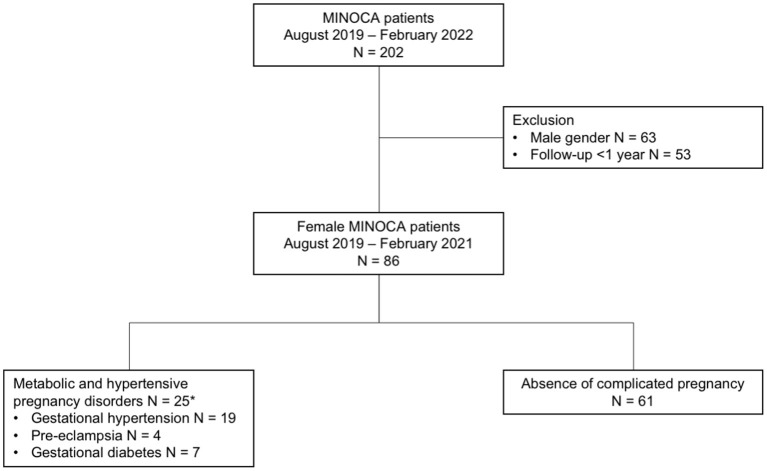
Methods: In this observational cohort study conducted at the Zuyderland Medical Center and Maastricht University Medical Center in the Netherlands, patients were enrolled if they were identified as having MINOCA. Data on individual patient characteristics, laboratory results, electrocardiography as well as (non-)invasive imaging procedures were derived from the electronic health record system. Patients were asked to complete a questionnaire about prior MHPD including GDM, GH, and PE. Patients were grouped into those with MHPD and those with prior uncomplicated normotensive pregnancy (or pregnancies; NP).
Results: After excluding patients without 1-year follow-up (n = 53), 86 female MINOCA patients remained eligible for analysis. Of the total female population, 25 (29.1%) patients had MHPD, including GH (n = 19; 22.1%), PE (n = 4; 4.7%), and GDM (n = 7; 8.1%). The MHPD patients showed higher rates of chronic hypertension (84.0 vs. 55.7%; p = 0.013), hypercholesterolemia (64.0 vs. 34.4%; p = 0.012), a family history of CVD (84.0 vs. 45.9%; p = 0.001), gout or rheumatic arthritis (16.0 vs. 1.6%; p = 0.024), and were more often non-smokers (45.8 vs. 78.3%; p = 0.004), compared to the NP patients. Moreover, MHPD patients were more likely to use cardiovascular medications at baseline. A trend toward no specific cause found for the MINOCA event was observed in MHPD patients compared to the NP group (64.0 vs. 42.6%, p = 0.072).
Conclusion: A history of metabolic and hypertensive pregnancy disorders occurred in one-third of female MINOCA patients. In these patients, conventional cardiovascular risk factors were more prevalent compared to NP patients. In most MHPD patients, the specific cause for MINOCA remained unclear.
Keywords: MINOCA; cardiovascular risk factor; gestational diabetes; gestational hypertension; preeclampsia.
Copyright © 2022 Pustjens, Vranken, Jansen, Winkler, Stein, Hoebers, Kietselaer, Spaanderman, Rasoul, Ghossein-Doha and van 't Hof.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Myocardial infarction without obstructive coronary artery disease (MINOCA) - prevalence and prognosis].Orv Hetil. 2019 Nov;160(45):1791-1797. doi: 10.1556/650.2019.31555. Orv Hetil. 2019. PMID: 31680539 Hungarian.
-
Clinical and electrocardiographic features of patients with myocardial infarction with non-obstructive coronary artery disease (MINOCA).J Cardiovasc Med (Hagerstown). 2021 Feb 1;22(2):104-109. doi: 10.2459/JCM.0000000000001027. J Cardiovasc Med (Hagerstown). 2021. PMID: 32706560
-
Myocardial infarction with non-obstructive coronary arteries (MINOCA) in Chinese patients: Clinical features, treatment and 1 year follow-up.Int J Cardiol. 2019 Jul 15;287:27-31. doi: 10.1016/j.ijcard.2019.02.036. Epub 2019 Feb 20. Int J Cardiol. 2019. PMID: 30826195
-
Myocardial infarction with non-obstructive coronary arteries: A comprehensive review and future research directions.World J Cardiol. 2019 Dec 26;11(12):305-315. doi: 10.4330/wjc.v11.i12.305. World J Cardiol. 2019. PMID: 31908730 Free PMC article. Review.
-
Myocardial infarction with non-obstructive coronary arteries (MINOCA): Intracoronary imaging-based diagnosis and management.J Cardiol. 2021 May;77(5):444-451. doi: 10.1016/j.jjcc.2021.01.001. Epub 2021 Jan 16. J Cardiol. 2021. PMID: 33468365 Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous