

Abnormal Diastolic Hemodynamic Forces: A Link Between Right Ventricular Wall Motion, Intracardiac Flow, and Pulmonary Regurgitation in Repaired Tetralogy of Fallot
- PMID: 35911535
- PMCID: PMC9329698
- DOI: 10.3389/fcvm.2022.929470
Abnormal Diastolic Hemodynamic Forces: A Link Between Right Ventricular Wall Motion, Intracardiac Flow, and Pulmonary Regurgitation in Repaired Tetralogy of Fallot
Abstract
Background and objective: The effect of chronic pulmonary regurgitation (PR) on right ventricular (RV) dysfunction in repaired Tetralogy of Fallot (RTOF) patients is well recognized by cardiac magnetic resonance (CMR). However, the link between RV wall motion, intracardiac flow and PR has not been established. Hemodynamic force (HDF) represents the global force exchanged between intracardiac blood volume and endocardium, measurable by 4D flow or by a novel mathematical model of wall motion. In our study, we used this novel methodology to derive HDF in a cohort of RTOF patients, exclusively using routine CMR imaging.
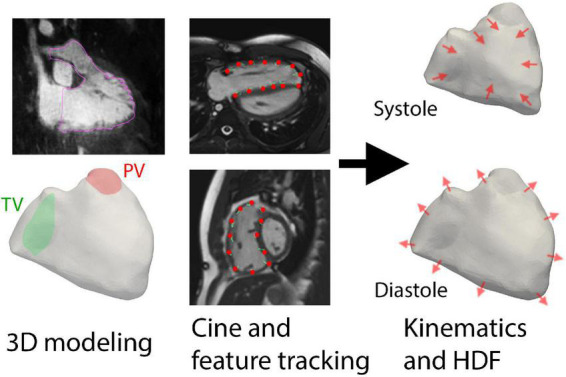
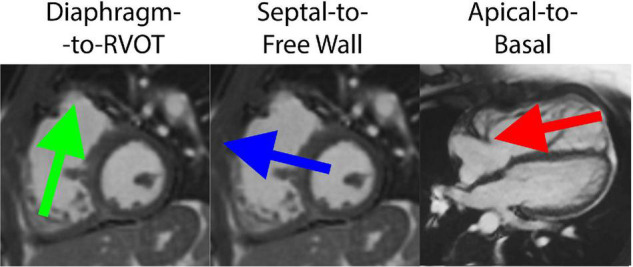
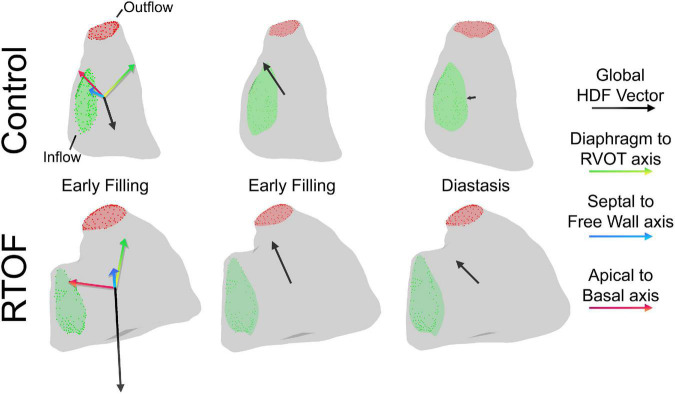
Methods: RTOF patients and controls with CMR imaging were retrospectively included. Three-dimensional (3D) models of RV were segmented, including RV outflow tract (RVOT). Feature-tracking software (QStrain 2.0, Medis Medical Imaging Systems, Leiden, Netherlands) captured endocardial contours from long/short-axis cine and used to reconstruct RV wall motion. A global HDF vector was computed from the moving surface, then decomposed into amplitude/impulse of three directional components based on reference (Apical-to-Basal, Septal-to-Free Wall and Diaphragm-to-RVOT direction). HDF were compared and correlated against CMR and exercise stress test parameters. A subset of RTOF patients had 4D flow that was used to derive vorticity (for correlation) and HDF (for comparison against cine method).
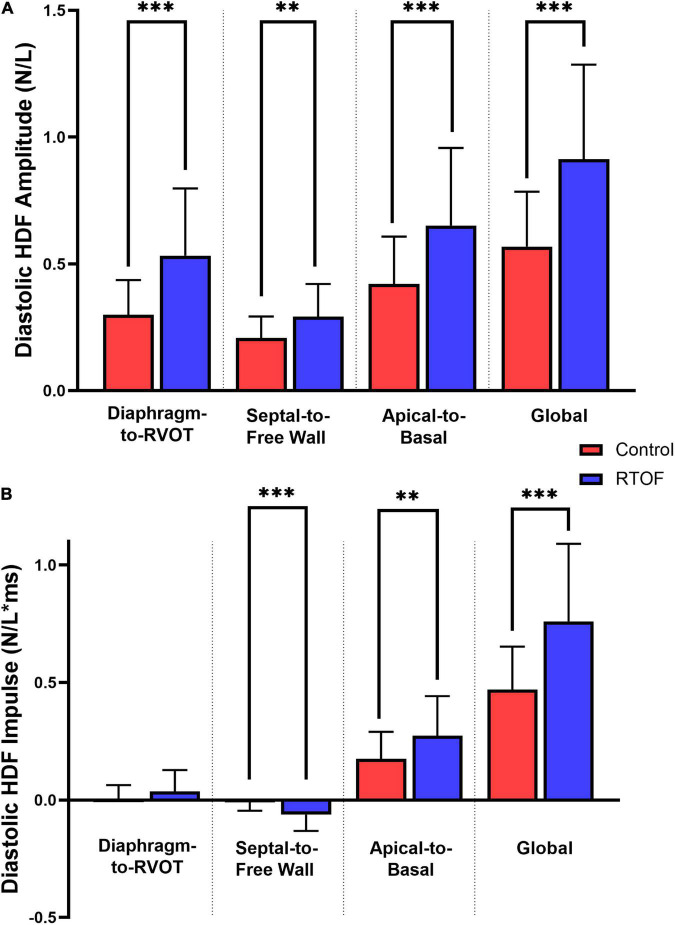
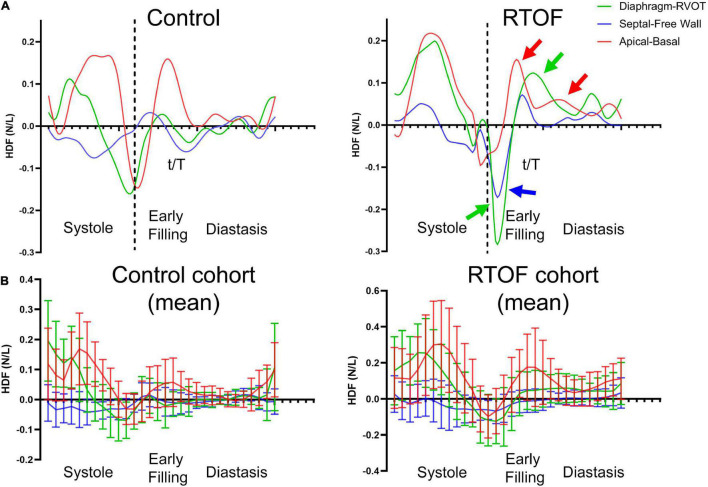
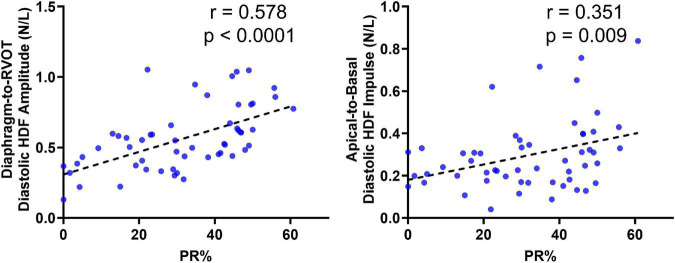
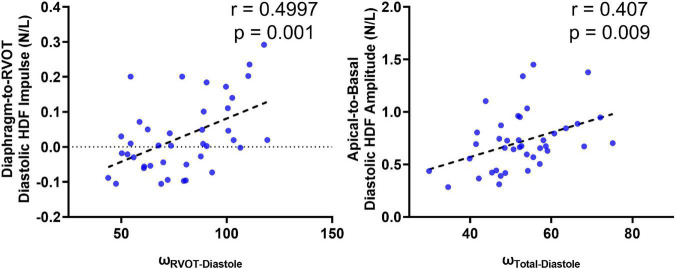
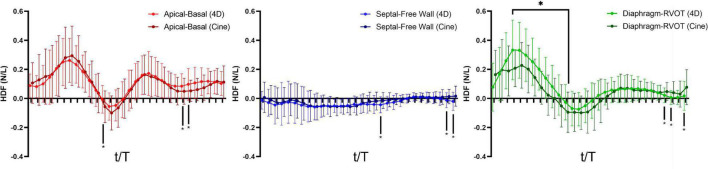
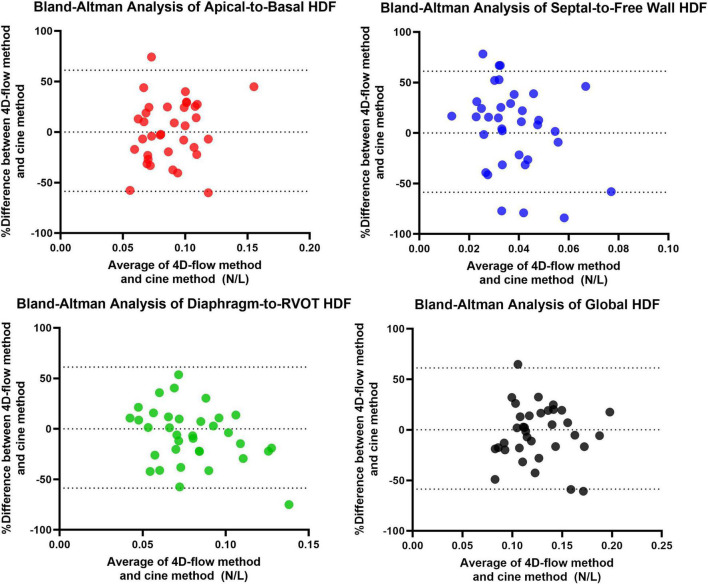
Results: 68 RTOF patients and 20 controls were included. RTOF patients had increased diastolic HDF amplitude in all three directions (p<0.05). PR% correlated with Diaphragm-RVOT HDF amplitude/impulse (r = 0.578, p<0.0001, r = 0.508, p < 0.0001, respectively). RV ejection fraction modestly correlated with global HDF amplitude (r = 0.2916, p = 0.031). VO2-max correlated with Septal-to-Free Wall HDF impulse (r = 0.536, p = 0.007). Diaphragm-to-RVOT HDF correlated with RVOT vorticity (r = 0.4997, p = 0.001). There was no significant measurement bias between Cine-derived HDF and 4D flow-derived HDF by Bland-Altman analysis.
Conclusion: RTOF patients have abnormal diastolic HDF that is correlated to PR, RV function, exercise capacity and vorticity. HDF can be derived from conventional cine, and is a potential link between RV wall motion and intracardiac flow from PR in RTOF patients.
Keywords: 4D flow; Tetralogy of Fallot; cardiac magnetic resonance; feature tracking; hemodynamic force.
Copyright © 2022 Loke, Capuano, Kollar, Cibis, Kitslaar, Balaras, Reiber, Pedrizzetti and Olivieri.
Conflict of interest statement
MC, PK, and JR were employed by Medis Medical Imaging Systems. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Statistical shape modeling reveals the link between right ventricular shape, hemodynamic force, and myocardial function in patients with repaired tetralogy of Fallot.Am J Physiol Heart Circ Physiol. 2022 Sep 1;323(3):H449-H460. doi: 10.1152/ajpheart.00228.2022. Epub 2022 Jul 15. Am J Physiol Heart Circ Physiol. 2022. PMID: 35839154 Free PMC article.
-
Moving beyond size: vorticity and energy loss are correlated with right ventricular dysfunction and exercise intolerance in repaired Tetralogy of Fallot.J Cardiovasc Magn Reson. 2021 Aug 19;23(1):98. doi: 10.1186/s12968-021-00789-2. J Cardiovasc Magn Reson. 2021. PMID: 34412634 Free PMC article.
-
Altered biventricular hemodynamic forces in patients with repaired tetralogy of Fallot and right ventricular volume overload because of pulmonary regurgitation.Am J Physiol Heart Circ Physiol. 2018 Dec 1;315(6):H1691-H1702. doi: 10.1152/ajpheart.00330.2018. Epub 2018 Sep 28. Am J Physiol Heart Circ Physiol. 2018. PMID: 30265559
-
Four-dimensional flow cardiac magnetic resonance assessment of left ventricular diastolic function.Front Cardiovasc Med. 2022 Jul 22;9:866131. doi: 10.3389/fcvm.2022.866131. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35935619 Free PMC article. Review.
-
Hemodynamic Force Based on Cardiac Magnetic Resonance Imaging: State of the Art and Perspective.J Magn Reson Imaging. 2025 Mar;61(3):1033-1047. doi: 10.1002/jmri.29483. Epub 2024 Jul 3. J Magn Reson Imaging. 2025. PMID: 38958118 Review.
Cited by
-
Assessing cardiac mechanics through left ventricular haemodynamic forces.Eur Heart J Imaging Methods Pract. 2024 Jul 25;2(3):qyae077. doi: 10.1093/ehjimp/qyae077. eCollection 2024 Jul. Eur Heart J Imaging Methods Pract. 2024. PMID: 39224620 Free PMC article. Review.
-
NLRP3 inflammasome activation by turbulent shear stress drives right ventricular outflow tract fibrosis in pulmonary regurgitation.Front Cardiovasc Med. 2025 May 2;12:1546581. doi: 10.3389/fcvm.2025.1546581. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40384971 Free PMC article.
-
Tetralogy of Fallot regurgitation energetics and kinetics: an intracardiac flow analysis of the right ventricle using computational fluid dynamics.Int J Cardiovasc Imaging. 2024 May;40(5):1135-1147. doi: 10.1007/s10554-024-03084-0. Epub 2024 Apr 26. Int J Cardiovasc Imaging. 2024. PMID: 38668927
-
Discordances in Kinetic Energy Between the Superior Cavopulmonary Connection and Single Ventricle Are Associated With Suboptimal Fontan Outcomes: A Pre-Fontan 4-Dimensional Flow Study.J Am Heart Assoc. 2025 Apr 15;14(8):e037949. doi: 10.1161/JAHA.124.037949. Epub 2025 Apr 3. J Am Heart Assoc. 2025. PMID: 40178094 Free PMC article.
-
Statistical shape modeling reveals the link between right ventricular shape, hemodynamic force, and myocardial function in patients with repaired tetralogy of Fallot.Am J Physiol Heart Circ Physiol. 2022 Sep 1;323(3):H449-H460. doi: 10.1152/ajpheart.00228.2022. Epub 2022 Jul 15. Am J Physiol Heart Circ Physiol. 2022. PMID: 35839154 Free PMC article.
References
-
- Loke YH, Capuano F, Cleveland V, Mandell JG, Balaras E, Olivieri LJ. Moving beyond size: vorticity and energy loss are correlated with right ventricular dysfunction and exercise intolerance in repaired Tetralogy of Fallot. J Cardiovasc Magn Reson. (2021) 23:98. 10.1186/s12968-021-00789-2 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials