

Mechanisms of Post-critical Illness Cardiovascular Disease
- PMID: 35911546
- PMCID: PMC9334745
- DOI: 10.3389/fcvm.2022.854421
Mechanisms of Post-critical Illness Cardiovascular Disease
Abstract
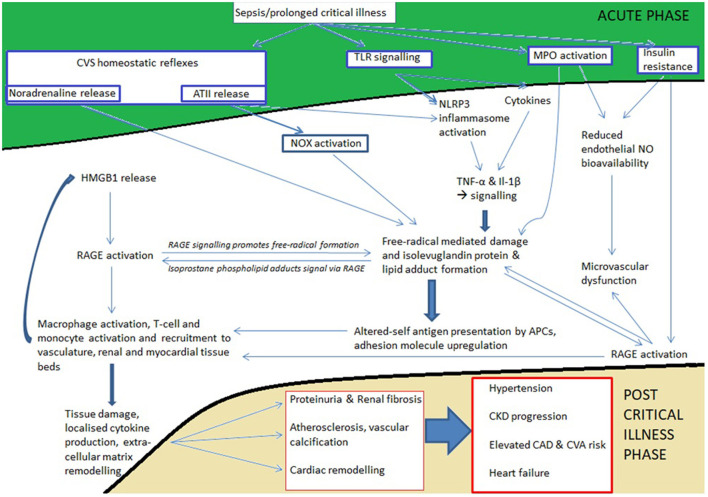
Prolonged critical care stays commonly follow trauma, severe burn injury, sepsis, ARDS, and complications of major surgery. Although patients leave critical care following homeostatic recovery, significant additional diseases affect these patients during and beyond the convalescent phase. New cardiovascular and renal disease is commonly seen and roughly one third of all deaths in the year following discharge from critical care may come from this cluster of diseases. During prolonged critical care stays, the immunometabolic, inflammatory and neurohumoral response to severe illness in conjunction with resuscitative treatments primes the immune system and parenchymal tissues to develop a long-lived pro-inflammatory and immunosenescent state. This state is perpetuated by persistent Toll-like receptor signaling, free radical mediated isolevuglandin protein adduct formation and presentation by antigen presenting cells, abnormal circulating HDL and LDL isoforms, redox and metabolite mediated epigenetic reprogramming of the innate immune arm (trained immunity), and the development of immunosenescence through T-cell exhaustion/anergy through epigenetic modification of the T-cell genome. Under this state, tissue remodeling in the vascular, cardiac, and renal parenchymal beds occurs through the activation of pro-fibrotic cellular signaling pathways, causing vascular dysfunction and atherosclerosis, adverse cardiac remodeling and dysfunction, and proteinuria and accelerated chronic kidney disease.
Keywords: CKD; atherosclerosis; chronicity; critical illness; heart failure; immune aging; inflammation; insulin resistance.
Copyright © 2022 Owen, Patel, Parekh and Bangash.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Mikkelsen ME, Still M, Anderson BJ, Bienvenu OJ, Brodsky MB, Brummel N, et al. . Society of critical care medicine's international consensus conference on prediction and identification of long-term impairments after critical illness. Crit Care Med. (2020) 48:1670–9. 10.1097/CCM.0000000000004586 - DOI - PubMed
-
- Arulkumaran N, Reay H, Brett SJ. on behalf of the JLA Intensive Care Research Priority Setting Partnership. Research priorities by professional background - a detailed analysis of the james lind alliance priority setting partnership. J Intensive Care Soc. (2016) 17:111–6. 10.1177/1751143715609954 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources