

Cardiac Magnetic Resonance in Rheumatology to Detect Cardiac Involvement Since Early and Pre-clinical Stages of the Autoimmune Diseases: A Narrative Review
- PMID: 35911548
- PMCID: PMC9326004
- DOI: 10.3389/fcvm.2022.870200
Cardiac Magnetic Resonance in Rheumatology to Detect Cardiac Involvement Since Early and Pre-clinical Stages of the Autoimmune Diseases: A Narrative Review
Abstract
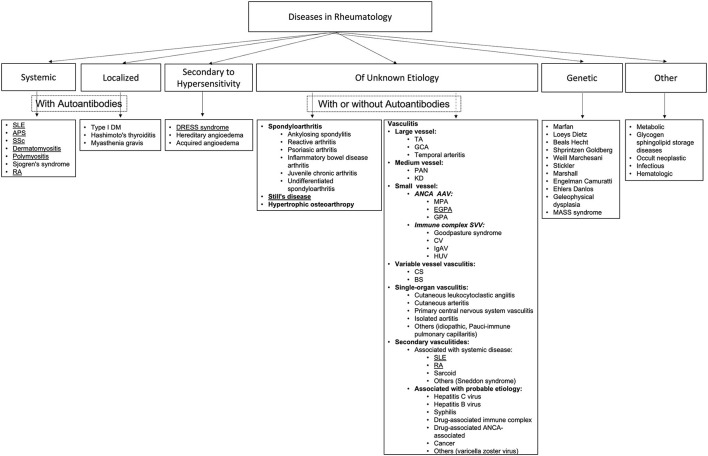
Autoimmune diseases (ADs) encompass multisystem disorders, and cardiovascular involvement is a well-known feature of autoimmune and inflammatory rheumatic conditions. Unfortunately, subclinical and early cardiovascular involvement remains clinically silent and often undetected, despite its well-documented impact on patient management and prognostication with an even more significant effect on severe and future MACE events as the disease progresses. Cardiac magnetic resonance imaging (MRI), today, commands a unique position of supremacy versus its competition in cardiac assessment and is the gold standard for the non-invasive evaluation of cardiac function, structure, morphology, tissue characterization, and flow with the capability of evaluating biventricular function; myocardium for edema, ischemia, fibrosis, infarction; valves for thickening, large masses; pericardial inflammation, pericardial effusions, and tamponade; cardiac cavities for thrombosis; conduction related abnormalities and features of microvascular and large vessel involvement. As precise and early detection of cardiovascular involvement plays a critical role in improving the outcome of rheumatic and autoimmune conditions, our review aims to highlight the evolving role of CMR in systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS), rheumatoid arthritis (RA), systemic sclerosis (SSc), limited sclerosis (LSc), adult-onset Still's disease (AOSD), polymyositis (PM), dermatomyositis (DM), eosinophilic granulomatosis with polyangiitis (EGPA) (formerly Churg-Strauss syndrome), and DRESS syndrome (DS). It draws attention to the need for concerted, systematic global interdisciplinary research to improve future outcomes in autoimmune-related rheumatic conditions with multiorgan, multisystem, and cardiovascular involvement.
Keywords: antiphospholipid; autoimmune disease; cardiac MRI; fibrosis; late gadolinium enhancement; lupus; rheumatoid arthritis; thrombosis.
Copyright © 2022 Sierra-Galan, Bhatia, Alberto-Delgado, Madrazo-Shiordia, Salcido, Santoyo, Martinez and Soto.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Comprehensive evaluation of cardiac involvement in eosinophilic granulomatosis with polyangiitis (EGPA) with cardiac magnetic resonance.Eur J Intern Med. 2017 Apr;39:51-56. doi: 10.1016/j.ejim.2016.09.014. Epub 2016 Oct 7. Eur J Intern Med. 2017. PMID: 27727077
-
The Critical Role of Cardiac Magnetic Resonance Imaging in Evaluating Patients With Eosinophilic Granulomatosis With Polyangiitis.Cureus. 2020 Sep 6;12(9):e10279. doi: 10.7759/cureus.10279. Cureus. 2020. PMID: 33042714 Free PMC article. Review.
-
Cardiovascular magnetic resonance imaging pattern at the time of diagnosis of treatment naïve patients with connective tissue diseases.Int J Cardiol. 2017 Jun 1;236:151-156. doi: 10.1016/j.ijcard.2017.01.104. Epub 2017 Feb 1. Int J Cardiol. 2017. PMID: 28185705
-
Detecting cardiac involvement with magnetic resonance in patients with active eosinophilic granulomatosis with polyangiitis.Int J Cardiovasc Imaging. 2016 Jun;32 Suppl 1:155-62. doi: 10.1007/s10554-016-0843-y. Epub 2016 Feb 1. Int J Cardiovasc Imaging. 2016. PMID: 26831057
-
Suspected inflammatory rheumatic diseases in patients presenting with skin rashes.Best Pract Res Clin Rheumatol. 2019 Aug;33(4):101440. doi: 10.1016/j.berh.2019.101440. Epub 2019 Oct 1. Best Pract Res Clin Rheumatol. 2019. PMID: 31585842 Review.
Cited by
-
Coexistent pleural effusion is found to be associated with aggravated subclinical myocardial injury in systemic lupus erythematous using cardiovascular magnetic resonance imaging.Front Immunol. 2024 Nov 25;15:1504624. doi: 10.3389/fimmu.2024.1504624. eCollection 2024. Front Immunol. 2024. PMID: 39654879 Free PMC article.
-
Cardiac Magnetic Resonance Imaging Findings in Patients With Antineutrophil Cytoplasmic Antibody-Associated Vasculitides: A Systematic Review.ACR Open Rheumatol. 2025 Apr;7(4):e70026. doi: 10.1002/acr2.70026. ACR Open Rheumatol. 2025. PMID: 40241489 Free PMC article. Review.
-
Exploring Cardiovascular Manifestations in Vasculitides: An In-Depth Review.Cureus. 2023 Aug 30;15(8):e44417. doi: 10.7759/cureus.44417. eCollection 2023 Aug. Cureus. 2023. PMID: 37791229 Free PMC article. Review.
-
Cutaneous Manifestations of Systemic Lupus Erythematosus and Their Correlation With Cardiac Involvement.Cureus. 2024 Dec 27;16(12):e76478. doi: 10.7759/cureus.76478. eCollection 2024 Dec. Cureus. 2024. PMID: 39866976 Free PMC article. Review.
-
Cardiac Magnetic Resonance-Detected Acute Myocardial Edema as Predictor of Favourable Prognosis: A Comprehensive Review.J Cardiovasc Dev Dis. 2023 Jul 27;10(8):319. doi: 10.3390/jcdd10080319. J Cardiovasc Dev Dis. 2023. PMID: 37623332 Free PMC article. Review.
References
-
- Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA, Friedrich MG, et al. . ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance. A Report of the American College of Cardiology foundation task force on expert consensus documents. J Am Coll Cardiol. (2010) 55:2614–62. 10.1016/j.jacc.2009.11.011 - DOI - PMC - PubMed
-
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. . 2021 ESC/EACTS Guidelines for the management of valvular heart disease: developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2021) 43:561–632. 10.1093/eurheartj/ehac051 - DOI - PubMed
-
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. . 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with. Eur Heart J. (2021) 42:3227–337. 10.1093/eurheartj/ehab484 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous