

Overstimulation of the ergoreflex-A possible mechanism to explain symptoms in long COVID
- PMID: 35911550
- PMCID: PMC9334659
- DOI: 10.3389/fcvm.2022.940832
Overstimulation of the ergoreflex-A possible mechanism to explain symptoms in long COVID
Abstract
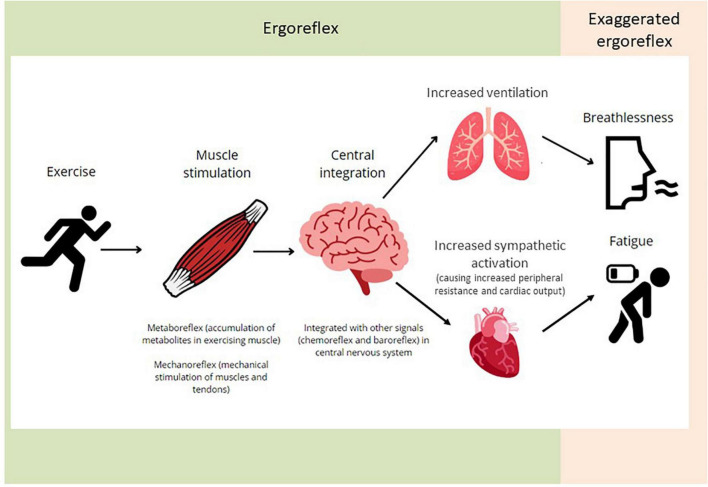
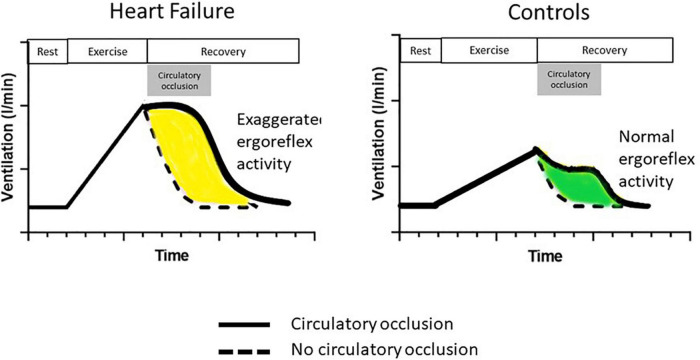
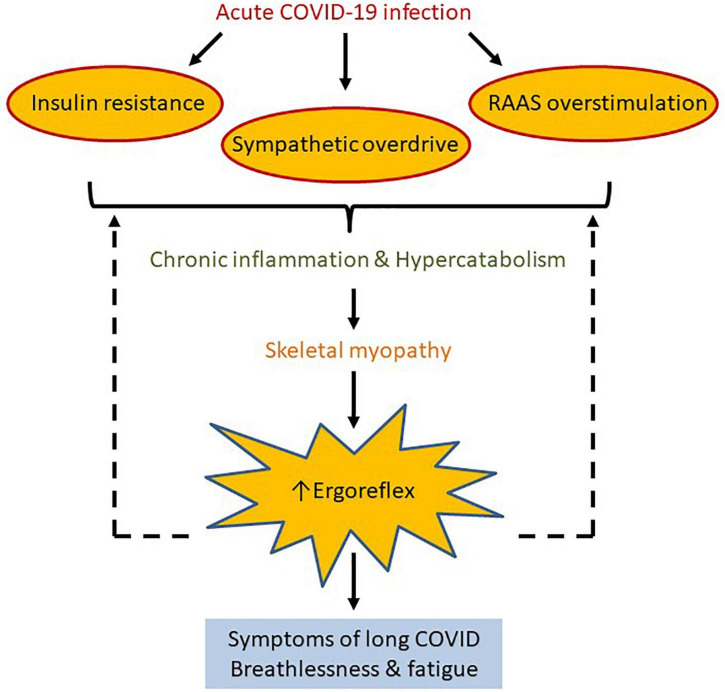
Long COVID refers to a multitude of symptoms that persist long after SARS-CoV-2 infection. Fatigue and breathlessness are the most common symptoms of long COVID across a range of studies. They are also cardinal symptoms of chronic heart failure (CHF). In this review, we propose that fatigue and breathlessness in patients with long COVID may be explained by skeletal muscle abnormalities, in a manner similar to patients with CHF. The ergoreflex is a cardiorespiratory reflex activated by exercise, which couples ventilation and cardiovascular function to exercise intensity. At least part of the symptomatology of CHF is related to abnormal skeletal muscle and an enhanced ergoreflex, resulting in heightened sympathetic, vasoconstrictor and ventilator drives. Similarly, SARS-CoV-2 infection results in a hyperinflammatory and hypercatabolic state. This leads to reduction in skeletal muscle mass and altered function. We postulate that the ergoreflex is chronically overstimulated, resulting in fatigue and breathlessness. Exercise training preserves muscle mass and function as well as reduces ergoreflex activation; therefore may have a role in improving symptoms associated with long COVID. Should the ergoreflex be proven to be an important pathophysiological mechanism of long COVID, tailored exercise interventions should be trialed with the aim of improving both symptoms and perhaps outcomes in patients with long COVID.
Keywords: breathlessness; ergoreflex; fatigue; heart failure; long COVID; pathophyisology.
Copyright © 2022 Sze, Pan, Moss, Ong, Pareek, Squire and Clark.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- NICE. Rapid Guideline Managing the Long Term Effects of Covid-19. London: NICE; (2022). p. 1–106.
-
- Rajan S, Khunti K, Alwan N, Steves C, MacDermott N, Morsella A, et al. In the Wake of the Pandemic: Preparing for Long COVID. Copenhagen: European Observatory on Health Systems and Policies; (2021). p. 1–27. - PubMed
-
- Evans RA, McAuley H, Harrison EM, Shikotra A, Singapuri A, Sereno M, et al. Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): a UK multicentre, prospective cohort study. Lancet Respir Med. (2021) 9:1275–87. 10.1016/S2213-2600(21)00383-0 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous