

Characteristics of Very High-Power, Short-Duration Radiofrequency Applications
- PMID: 35911564
- PMCID: PMC9326019
- DOI: 10.3389/fcvm.2022.941434
Characteristics of Very High-Power, Short-Duration Radiofrequency Applications
Abstract
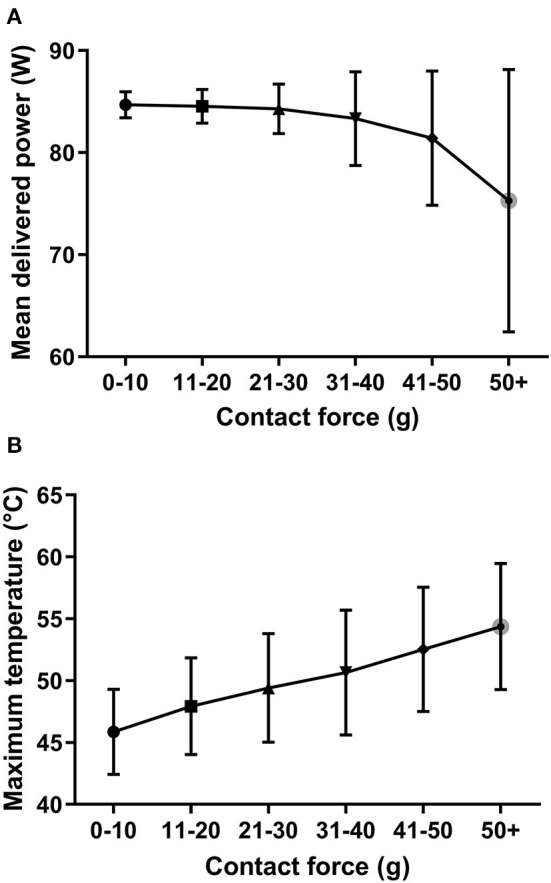
Introduction: Pulmonary vein isolation is the cornerstone of rhythm-control therapy for atrial fibrillation (AF). The very high-power, short-duration (vHPSD) radiofrequency (RF) ablation is a novel technology that favors resistive heating while decreasing the role of conductive heating. Our study aimed to evaluate the correlations between contact force (CF), power, impedance drop (ID), and temperature; and to assess their role in lesion formation with the vHPSD technique.
Methods: Consecutive patients who underwent initial point-by-point RF catheter ablation for AF were enrolled in the study. The vHPSD ablation was performed applying 90 W for 4 s with an 8 ml/min irrigation rate.
Results: Data from 85 patients [median age 65 (59-71) years, 34% female] were collected. The median procedure time, left atrial dwelling time, and fluoroscopy time were 70 (60-90) min, 49 (42-58) min, and 7 (5-11) min, respectively. The median RF time was 312 (237-365) sec. No steam pop nor major complications occurred. A total of 6,551 vHPSD RF points were analyzed. The median of CF, maximum temperature, and ID were 14 (10-21) g, 47.6 (45.1-50.4) °C, and 8 (6-10) Ohms, respectively. CF correlated significantly with the maximum temperature (p < 0.0001). A CF of 5 g and above was associated with a significantly higher temperature compared to those lesions with a CF below 5 grams (p < 0.0001). Bilateral first-pass isolation rate was 84%. The 6-month AF-recurrence rate was 7%.
Conclusion: The maximum temperature and CF significantly correlate with each other during vHPSD applications. A CF ≥ 5 g leads to better tissue heating and thus might be more likely to result in good lesion formation, although this clinical study was unable to assess actual lesion sizes.
Keywords: ablation; atrial fibrillation; pulmonary vein isolation; short duration; very high power.
Copyright © 2022 Orbán, Salló, Perge, Ábrahám, Piros, Nagy, Osztheimer, Merkely, Gellér and Szegedi.
Conflict of interest statement
NS, ZS, and LG report consulting fees from Biosense Webster, not related to the present work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. . 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European association for cardio-thoracic surgery (EACTS). Eur Heart J. (2021) 42:373–498. 10.1093/eurheartj/ehaa612 - DOI - PubMed
-
- Nielsen JC, Johannessen A, Raatikainen P, Hindricks G, Walfridsson H, Pehrson SM, et al. . Long-term efficacy of catheter ablation as first-line therapy for paroxysmal atrial fibrillation: 5-year outcome in a randomised clinical trial. Heart. (2017) 103:368–76. 10.1136/heartjnl-2016-309781 - DOI - PubMed
-
- Arbelo E, Brugada J, Blomström-Lundqvist C, Laroche C, Kautzner J, Pokushalov E, et al. . Contemporary management of patients undergoing atrial fibrillation ablation: in-hospital and 1-year follow-up findings from the ESC-EHRA atrial fibrillation ablation long-term registry. Eur Heart J. (2017) 38:1303–16. 10.1093/eurheartj/ehw564 - DOI - PubMed
LinkOut - more resources
Full Text Sources