

Diagnostic Value of Multimodal Magnetic Resonance Imaging in Discriminating Between Metastatic and Non-Metastatic Pelvic Lymph Nodes in Cervical Cancer
- PMID: 35911622
- PMCID: PMC9326496
- DOI: 10.2147/IJGM.S372154
Diagnostic Value of Multimodal Magnetic Resonance Imaging in Discriminating Between Metastatic and Non-Metastatic Pelvic Lymph Nodes in Cervical Cancer
Abstract
Background: The status of pelvic lymph node (PLN) metastasis affects treatment and prognosis plans in patients with cervical cancer. However, it is hard to be diagnosed in clinical practice.
Purpose: The present study aimed to evaluate the diagnostic value of multimodal magnetic resonance imaging (MRI) in discriminating between metastatic and non-metastatic pelvic lymph nodes (PLNs) in cervical cancer.
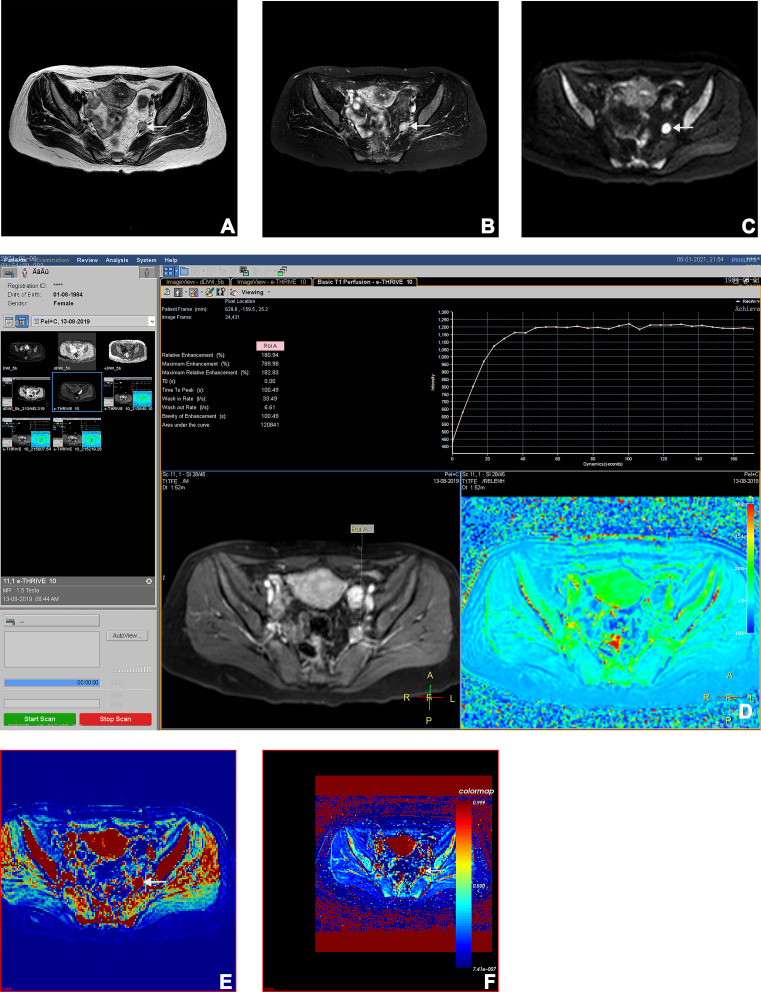
Methods: This retrospective study analyzed MRIs of 209 PLNs in 25 women with pathologically proven cervical cancer. All PLNs had been assessed by pre-treatment multimodal MRIs, and their status was finally confirmed by histopathology. In conventional MRI, lymph node characteristics were compared between metastatic and non-metastatic PLNs. Signal intensity, time-intensity curve (TIC) patterns minimal and mean apparent diffusion coefficients (ADC) were compared between them in DWI. In DCE-MRI, quantitative (Ktrans, Kep and Ve) analyses were performed on DCE-MRI sequences, and their predictive values were analyzed by ROC curves.
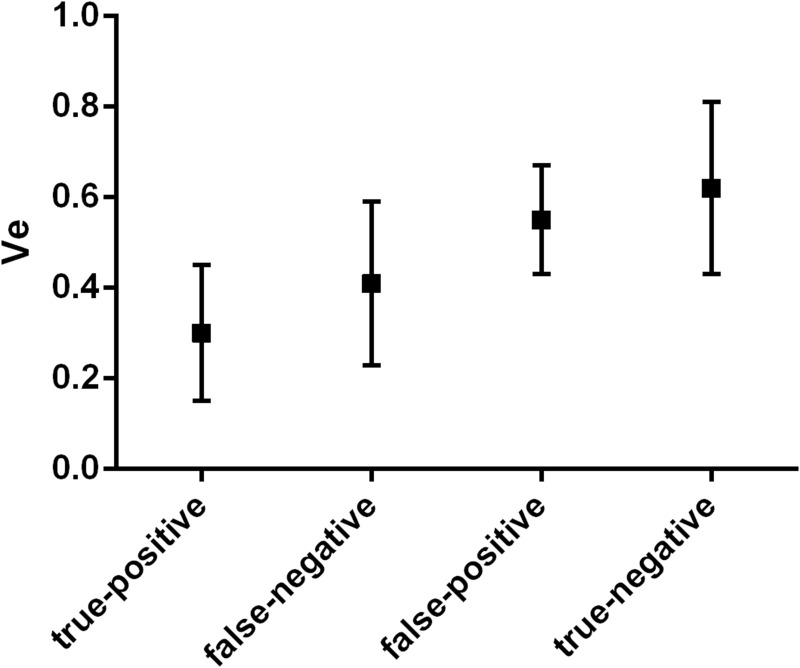
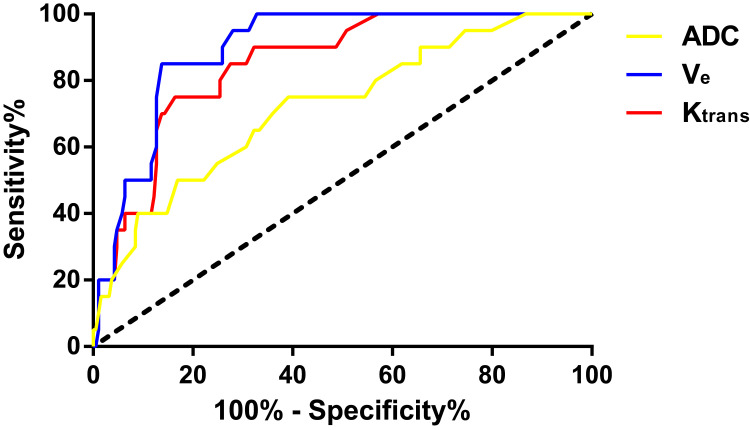
Results: Of 209 PLNs, 22 (10.53%) were metastases and 187 (89.47%) were non-metastases at histopathologic examination. Considering a comparison of lymph node characteristics, the short axis size, the long axis size, and the boundary differed significantly between the two groups (P<0.05).The differences in ADCmin, TIC types, Ktrans and Ve between metastatic and non-metastatic PLNs were significant as well (P<0.05). The good diagnostic performance of multimodal MRI was shown in discriminating between metastatic and non-metastatic PLNs, with the sensitivity of 85.0% (17/20), specificity of 97.3% (184/189), and accuracy of 96.2% (201/209). ROC analyses showed that the diagnostic accuracy of ADCmin, Ktrans and Ve for discriminating between metastatic and non-metastatic PLNs in cervical cancer was 83.7%, 91.4%, and 92.4% with the cut-off values of 0.72 × 10-3mm2/s, 0.52 min-1, and 0.53 min-1, respectively.
Conclusion: Multimodal MRI showed good diagnostic performance in determining PLN status in cervical cancer.
Keywords: apparent diffusion coefficient; cervical cancer; lymphatic metastasis; multimodal magnetic resonance imaging.
© 2022 Xu et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures



Similar articles
-
Diagnostic value of diffusion-weighted magnetic resonance imaging in discriminating between metastatic and non-metastatic pelvic lymph nodes in endometrial cancer.Acta Radiol. 2020 Nov;61(11):1580-1586. doi: 10.1177/0284185120906660. Epub 2020 Feb 27. Acta Radiol. 2020. PMID: 32106683
-
Application of apparent diffusion coefficient values derived from diffusion-weighted imaging for assessing different sized metastatic lymph nodes in cervical cancers.Acta Radiol. 2020 Jun;61(6):848-855. doi: 10.1177/0284185119879686. Epub 2019 Oct 15. Acta Radiol. 2020. PMID: 31615267
-
The Role of Multiparametric Magnetic Resonance Imaging in the Study of Primary Tumor and Pelvic Lymph Node Metastasis in Stage IB1-IIA1 Cervical Cancer.J Comput Assist Tomogr. 2020 Sep/Oct;44(5):750-758. doi: 10.1097/RCT.0000000000001084. J Comput Assist Tomogr. 2020. PMID: 32842062
-
Apparent diffusion coefficient magnetic resonance imaging (ADC-MRI) in the axillary breast cancer lymph node metastasis detection: a narrative review.Gland Surg. 2020 Dec;9(6):2225-2234. doi: 10.21037/gs-20-546. Gland Surg. 2020. PMID: 33447575 Free PMC article. Review.
-
Pancreatic draining lymph nodes (PLNs) serve as a pathogenic hub contributing to the development of type 1 diabetes.Cell Biosci. 2023 Aug 28;13(1):156. doi: 10.1186/s13578-023-01110-7. Cell Biosci. 2023. PMID: 37641145 Free PMC article. Review.
Cited by
-
Prognostic analysis of patients with stage IIIC1p cervical cancer treated by surgery.World J Surg Oncol. 2023 Jun 21;21(1):186. doi: 10.1186/s12957-023-03076-9. World J Surg Oncol. 2023. PMID: 37344912 Free PMC article.
-
The value of multiparameter MRI of early cervical cancer combined with SCC-Ag in predicting its pelvic lymph node metastasis.Front Oncol. 2024 Sep 11;14:1417933. doi: 10.3389/fonc.2024.1417933. eCollection 2024. Front Oncol. 2024. PMID: 39323994 Free PMC article.
-
Tumor markers and multimodal magnetic resonance imaging in predicting rectal cancer stage and differentiation.World J Gastrointest Oncol. 2025 Aug 15;17(8):108007. doi: 10.4251/wjgo.v17.i8.108007. World J Gastrointest Oncol. 2025. PMID: 40837746 Free PMC article.
-
Machine Learning-Based Multiparametric Magnetic Resonance Imaging Radiomics Model for Preoperative Predicting the Deep Stromal Invasion in Patients with Early Cervical Cancer.J Imaging Inform Med. 2024 Feb;37(1):230-246. doi: 10.1007/s10278-023-00906-w. Epub 2024 Jan 10. J Imaging Inform Med. 2024. PMID: 38343218 Free PMC article.
References
-
- Cohen PA, Jhingran A, Oaknin A, Denny L. Cervical cancer. Lancet. 2019;393(10167):169–182. - PubMed
-
- Thomassin-Naggara I, Bazot M, Daraï E, Callard P, Thomassin J, Cuenod CA. Epithelial ovarian tumors: value of dynamic contrast-enhanced MR imaging and correlation with tumor angiogenesis. Radiology. 2008;248(1):148–159. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
