

Placental Malaria is Associated with Higher LILRB2 Expression in Monocyte Subsets and Lower Anti-Malarial IgG Antibodies During Infancy
- PMID: 35911674
- PMCID: PMC9326509
- DOI: 10.3389/fimmu.2022.909831
Placental Malaria is Associated with Higher LILRB2 Expression in Monocyte Subsets and Lower Anti-Malarial IgG Antibodies During Infancy
Abstract
Background: Placental malaria (PM) is associated with a higher susceptibility of infants to Plasmodium falciparum (Pf) malaria. A hypothesis of immune tolerance has been suggested but no clear explanation has been provided so far. Our goal was to investigate the involvement of inhibitory receptors LILRB1 and LILRB2, known to drive immune evasion upon ligation with pathogen and/or host ligands, in PM-induced immune tolerance.
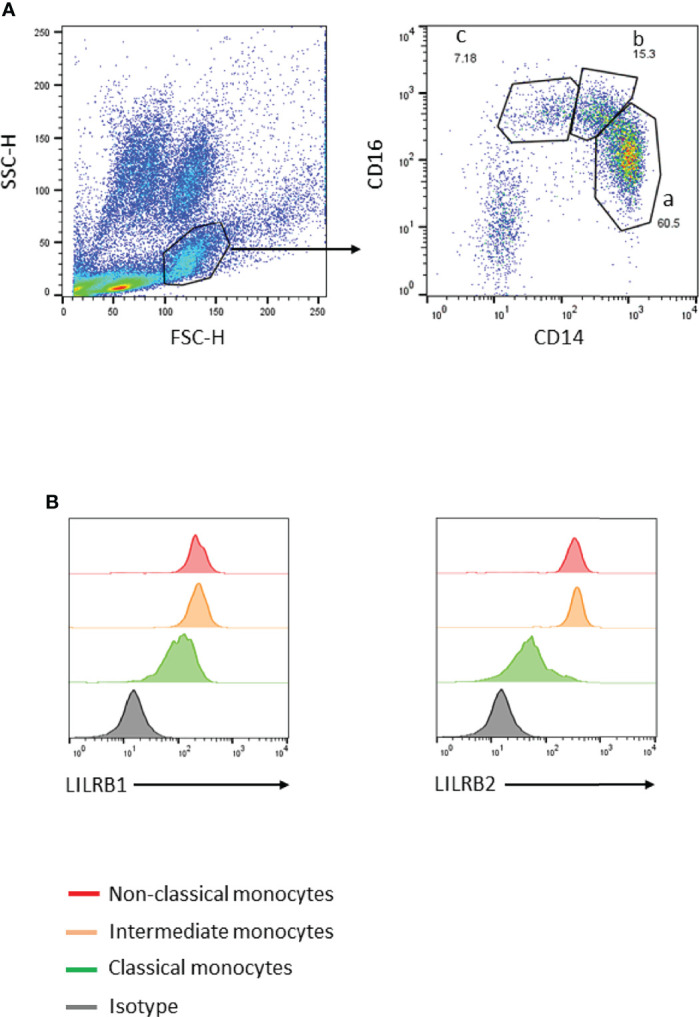
Method: Infants of women with or without PM were enrolled in Allada, southern Benin, and followed-up for 24 months. Antibodies with specificity for five blood stage parasite antigens were quantified by ELISA, and the frequency of immune cell subsets was quantified by flow cytometry. LILRB1 or LILRB2 expression was assessed on cells collected at 18 and 24 months of age.
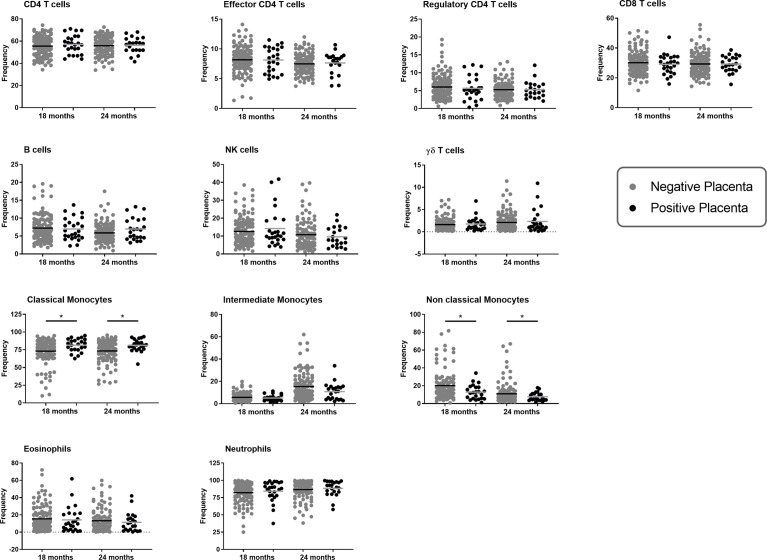
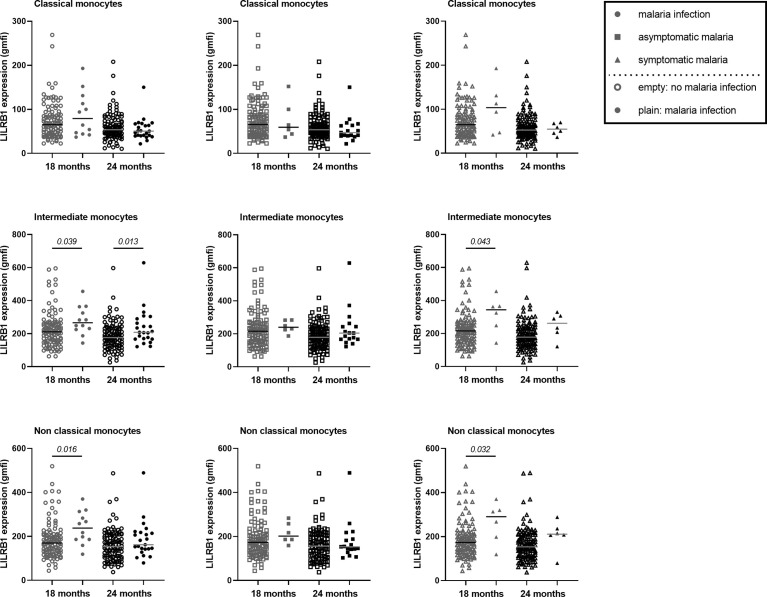
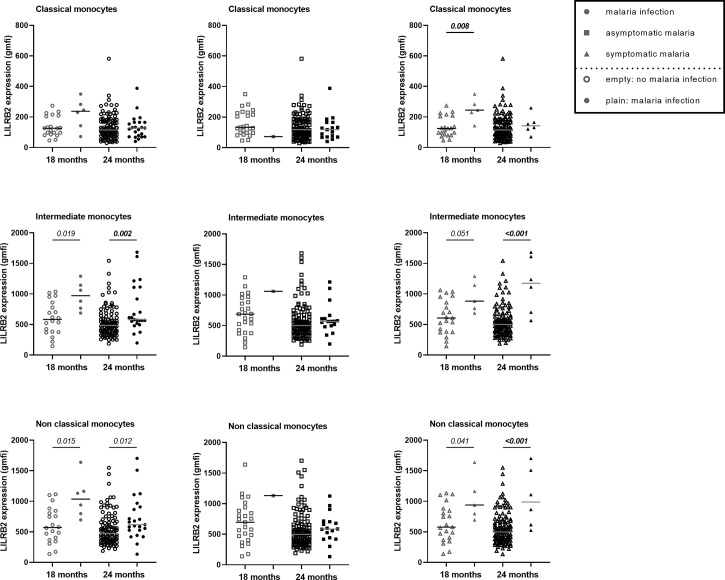
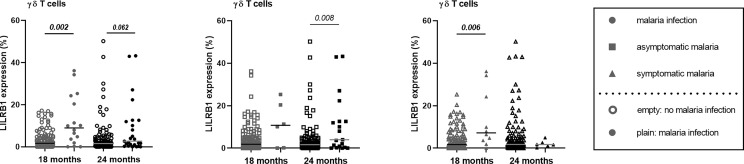
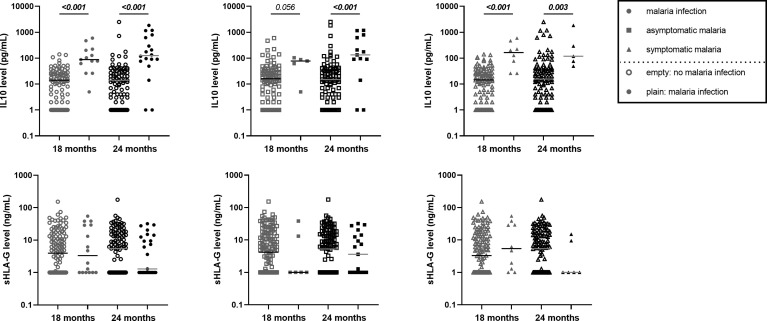
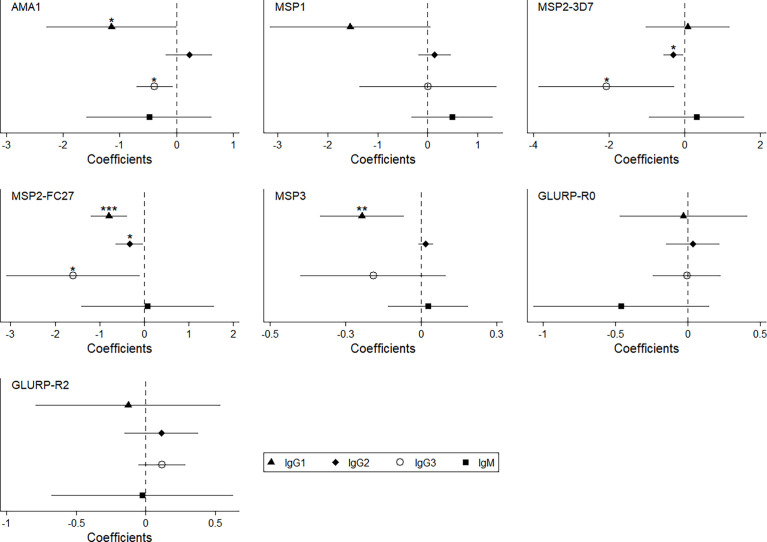
Findings: Infants born to women with PM had a higher risk of developing symptomatic malaria than those born to women without PM (IRR=1.53, p=0.040), and such infants displayed a lower frequency of non-classical monocytes (OR=0.74, p=0.01) that overexpressed LILRB2 (OR=1.36, p=0.002). Moreover, infants born to women with PM had lower levels of cytophilic IgG and higher levels of IL-10 during active infection.
Interpretation: Modulation of IgG and IL-10 levels could impair monocyte functions (opsonisation/phagocytosis) in infants born to women with PM, possibly contributing to their higher susceptibility to malaria. The long-lasting effect of PM on infants' monocytes was notable, raising questions about the capacity of ligands such as Rifins or HLA-I molecules to bind to LILRB1 and LILRB2 and to modulate immune responses, and about the reprogramming of neonatal monocytes/macrophages.
Keywords: Gd T cell; HLA-G; LILRB1; LILRB2; Plasmodium falciparum; immune tolerance; malaria candidate vaccine; monocytes.
Copyright © 2022 Dechavanne, Nouatin, Adamou, Edslev, Hansen, Meurisse, Sadissou, Gbaguidi, Milet, Cottrell, Gineau, Sabbagh, Massougbodji, Moutairou, Donadi, Carosella, Moreau, Remarque, Theisen, Rouas-Freiss, Garcia, Favier and Courtin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials