

Subclinical Magnetic Resonance Imaging Markers of Cerebral Small Vessel Disease in Relation to Office and Ambulatory Blood Pressure Measurements
- PMID: 35911921
- PMCID: PMC9330602
- DOI: 10.3389/fneur.2022.908260
Subclinical Magnetic Resonance Imaging Markers of Cerebral Small Vessel Disease in Relation to Office and Ambulatory Blood Pressure Measurements
Abstract
Background: Twenty-four-hour and nighttime blood pressure (BP) levels are more strongly associated with cardiovascular risk than office or daytime BP measurements. However, it remains undocumented which of the office and ambulatory BP measurements have the strongest association and predictive information in relation to the presence of type I, or arteriolosclerosis type, cerebral small vessel diseases (CSVD).
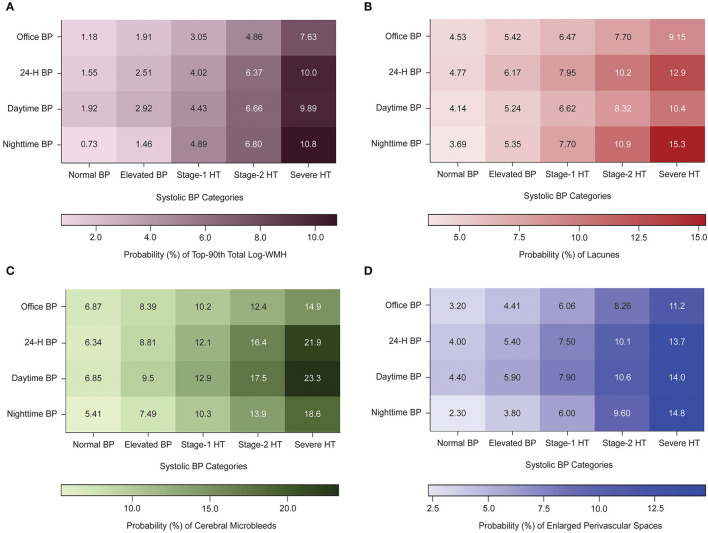
Methods: A subset of 429 participants from the Maracaibo Aging Study [aged ≥40 years (women, 73.7%; mean age, 59.3 years)] underwent baseline brain magnetic resonance imaging (MRI) to visualize CSVD, which included log-transformed white matter hyperintensities (log-WMH) volume and the presence (yes/no) of lacunes, cerebral microbleeds (CMB), or enlarged perivascular spaces (EPVS). Linear and logistic regression models were applied to examine the association between CSVD and each +10-mmHg increment in the office and ambulatory systolic BP measurements. Improvement in the fit of nested logistic models was assessed by the log-likelihood ratio and the generalized R 2 statistic.
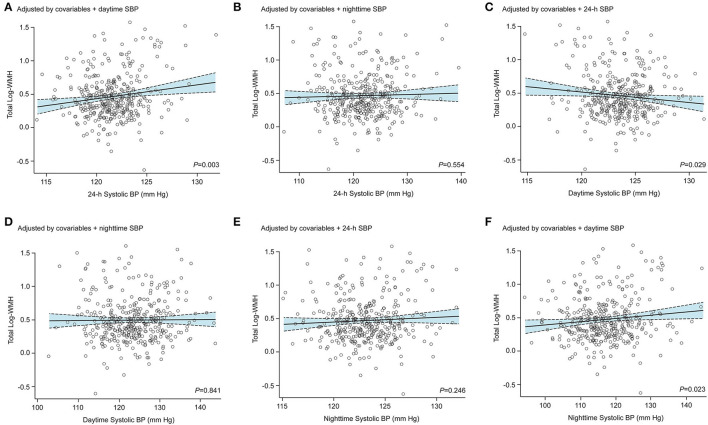
Results: Office and ambulatory systolic BP measurements were related to log-WMH (β-correlation coefficients ≥0.08; P < 0.001). Lacunes and CMB were only associated with ambulatory systolic BP measurements (odds ratios [OR] ranged from 1.31 [95% confidence interval, 1.10-1.55] to 1.46 [1.17-1.84], P ≤ 0.003). Accounted for daytime systolic BP, both the 24-h (β-correlation, 0.170) and nighttime (β-correlation, 0.038) systolic BP measurements remained related to log-WMH. When accounted for 24-h or daytime systolic BP levels, the nighttime systolic BP retained the significant association with lacunes (ORs, 1.05-1.06; 95% CIs, ≥1.01 to ≤ 1.13), whereas the 24-h and daytime systolic BP levels were not associated with lacunes after adjustments for nighttime systolic BP (ORs, ≤ 0.88; 95% CI, ≥0.77 to ≤ 1.14). On top of covariables and office systolic BP, ambulatory systolic BP measurements significantly improved model performance (1.05% ≥ R 2 ≤ 3.82%). Compared to 24-h and daytime systolic BP, nighttime systolic BP had the strongest improvement in the model performance; for WMH (1.46 vs. 1.05%) and lacunes (3.06 vs. ≤ 2.05%).
Conclusions: Twenty-four-hour and nighttime systolic BP were the more robust BP measurements associated with CSVD, but the nighttime systolic BP level had the strongest association. Controlling ambulatory BP levels might provide additional improvement in the prevention of CSVD.
Keywords: ambulatory blood pressure monitoring; cerebral microbleeds; cerebral small vessel disease; enlarged perivascular spaces; lacunes; nighttime blood pressure; white matter hyperintensities.
Copyright © 2022 Melgarejo, Maestre, Gutierrez, Thijs, Mena, Gaona, Leendertz, Lee, Chávez, Calmon, Silva, Wei, Terwilliger, Vanassche, Janssens, Verhamme, Bos and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Correlation of blood pressure levels at different time periods throughout the day with total CSVD burden and MRI imaging markers.Front Neurol. 2023 Jul 25;14:1200846. doi: 10.3389/fneur.2023.1200846. eCollection 2023. Front Neurol. 2023. PMID: 37576008 Free PMC article.
-
Ambulatory Blood Pressure Levels in the Prediction of Progression of Cerebral Small Vessel Disease.J Am Geriatr Soc. 2020 Oct;68(10):2232-2239. doi: 10.1111/jgs.16568. Epub 2020 Jun 8. J Am Geriatr Soc. 2020. PMID: 32511756
-
Intracranial Carotid Arteriosclerosis Mediates the Association Between Blood Pressure and Cerebral Small Vessel Disease.Hypertension. 2023 Mar;80(3):618-628. doi: 10.1161/HYPERTENSIONAHA.122.20434. Epub 2022 Dec 2. Hypertension. 2023. PMID: 36458543 Free PMC article.
-
Correlations of Plasma Biomarkers and Imaging Characteristics of Cerebral Small Vessel Disease.Brain Sci. 2024 Mar 12;14(3):269. doi: 10.3390/brainsci14030269. Brain Sci. 2024. PMID: 38539657 Free PMC article. Review.
-
Blood Pressure Variability and Cerebral Small Vessel Disease: A Systematic Review and Meta-Analysis of Population-Based Cohorts.Stroke. 2020 Jan;51(1):82-89. doi: 10.1161/STROKEAHA.119.026739. Epub 2019 Nov 27. Stroke. 2020. PMID: 31771460 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources