

Case Report: Monoclonal Gammopathies of Clinical Significance-Associated Myopathy: A Case-Based Review
- PMID: 35912259
- PMCID: PMC9333131
- DOI: 10.3389/fonc.2022.914379
Case Report: Monoclonal Gammopathies of Clinical Significance-Associated Myopathy: A Case-Based Review
Abstract
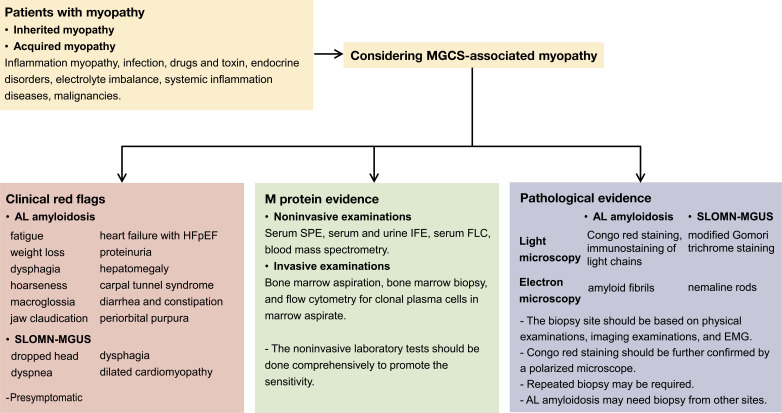
Monoclonal gammopathies of clinical significance (MGCS)-associated myopathy is a group of muscular MGCS-based rare manifestations. It mainly includes amyloid light chain (AL) amyloidosis and sporadic late-onset nemaline myopathy with monoclonal gammopathy of undetermined significance. When myopathy manifests as the initial or sole clinical symptom, it can often be delayed or misdiagnosed as other myopathies. We report the case of a 60-year-old man who initially presented with fatigue and muscle weakness of the symmetric proximal lower limbs. Muscle biopsy did not reveal mononuclear cell infiltration, atrophy, necrosis, or positive Congo red staining results. The results of serum protein electrophoresis and immunofixation electrophoresis were negative. No specific diagnosis was established. After 1 year, the patient was diagnosed with AL amyloidosis after myocardial and fat pad biopsies were performed and myopathy was diagnosed as AL amyloidosis-associated myopathy after reassessment. The patient received CyBorD regime chemotherapy and achieved hematological and organ remission. Therefore, we reviewed the clinical and pathological manifestations of MGCS-associated myopathies. Based on published articles and the present case, we conclude that comprehensive screening for MGCS in unexplained myopathy is essential to avoid misdiagnosis or delayed diagnosis.
Keywords: MGCS; MGUS; amyloidosis; myopathy; nemaline myopathy.
Copyright © 2022 Yu, He, Zhang, Cao, Liu and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Lundberg IE, Tjärnlund A, Bottai M, Werth VP, Pilkington C, de Visser M, et al. . European League Against Rheumatism/American College of Rheumatology Classification Criteria for Adult and Juvenile Idiopathic Inflammatory Myopathies and Their Major Subgroups. Arthritis Rheumatol (2017) 69(12):2271–82. doi: 10.1002/art.40320 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources