

A comparison of agreement between actigraphy and polysomnography for assessing sleep during posttraumatic amnesia
- PMID: 35912692
- PMCID: PMC9622995
- DOI: 10.5664/jcsm.10174
A comparison of agreement between actigraphy and polysomnography for assessing sleep during posttraumatic amnesia
Abstract
Study objectives: Sleep disturbance often emerges in the early recovery phase following a moderate to severe traumatic brain injury, known as posttraumatic amnesia. Actigraphy is commonly employed to assess sleep, as it is assumed that patients in posttraumatic amnesia (who display confusion, restlessness, and agitation) would better tolerate this measure over gold-standard polysomnography (PSG). This study evaluated the agreement between PSG and actigraphy for determining (sleep/wake time, sleep efficiency, sleep latency, and awakenings) in patients experiencing posttraumatic amnesia. It also compared the epoch-by-epoch sensitivity, specificity, and accuracy between the Actigraph device's 4 wake threshold settings (low, medium, high, and automatic) to PSG.
Methods: The sample consisted of 24 inpatients recruited from a traumatic brain injury inpatient rehabilitation unit. Ambulatory PSG was recorded overnight at bedside and a Philips Actiwatch was secured to each patient's wrist for the same period.
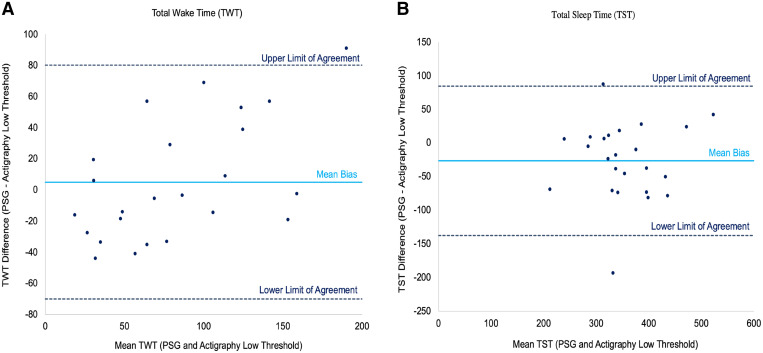
Results: There were poor correlations between PSG and actigraphy for all parameters (Lin's concordance correlation coefficient = < 0.80). The low threshold displayed the highest correlation with PSG for wake and sleep time, albeit still low. Actigraphy displayed low specificity (ranging from 17.1% to 36.6%). There appears to be a greater disparity between actigraphy and PSG for patients with increased wake time.
Conclusions: Actigraphy, while convenient, demonstrated poorer performance in determining sleep-wake parameters in patients with significantly disturbed sleep. Ambulatory PSG can provide a clearer understanding of the extent of sleep disturbances in these patients with reduced mobility during early rehabilitation. Study findings can help design future protocols of sleep assessment during posttraumatic amnesia and optimize treatment.
Citation: Fedele B, McKenzie D, Williams G, Giles R, Olver J. A comparison of agreement between actigraphy and polysomnography for assessing sleep during posttraumatic amnesia. J Clin Sleep Med. 2022;18(11):2605-2616.
Keywords: actigraphy; brain injuries; polysomnography; rehabilitation; sleep; traumatic.
© 2022 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have seen and approved this manuscript. Work for this study was performed at Department of Rehabilitation, Epworth HealthCare, 89 Bridge Road, Richmond, Victoria, 3121, Australia. This study was funded by the Professor Jack Cade AM Intensivist Major Development Grant from the Epworth Research Institute (ERI) and the Epworth Medical Foundation Grant Family Bequest. These grants provided the study equipment and staffing support outside the study team. The authors report no conflicts of interest.
Figures
Comment in
-
Poor agreement between actigraphy and polysomnography for assessing sleep during post-traumatic amnesia.J Clin Sleep Med. 2023 Jan 1;19(1):201. doi: 10.5664/jcsm.10318. J Clin Sleep Med. 2023. PMID: 36123950 Free PMC article. No abstract available.
-
Sleep assessment during early amnesic brain injury recovery.J Clin Sleep Med. 2023 Jan 1;19(1):203-204. doi: 10.5664/jcsm.10326. J Clin Sleep Med. 2023. PMID: 36239050 Free PMC article. No abstract available.
Similar articles
-
Sleep Disturbance During Post-Traumatic Amnesia and Early Recovery After Traumatic Brain Injury.J Neurotrauma. 2024 Aug;41(15-16):e1961-e1975. doi: 10.1089/neu.2023.0656. Epub 2024 May 6. J Neurotrauma. 2024. PMID: 38553904
-
Assessing Sleep Architecture With Polysomnography During Posttraumatic Amnesia After Traumatic Brain Injury: A Pilot Study.Neurorehabil Neural Repair. 2021 Jul;35(7):622-633. doi: 10.1177/15459683211011241. Epub 2021 May 12. Neurorehabil Neural Repair. 2021. PMID: 33978535
-
Utility of the Fitbit Flex to evaluate sleep in major depressive disorder: A comparison against polysomnography and wrist-worn actigraphy.J Affect Disord. 2017 Aug 1;217:299-305. doi: 10.1016/j.jad.2017.04.030. Epub 2017 Apr 19. J Affect Disord. 2017. PMID: 28448949 Free PMC article.
-
Sleep and agitation during subacute traumatic brain injury rehabilitation: A scoping review.Aust Crit Care. 2021 Jan;34(1):76-82. doi: 10.1016/j.aucc.2020.05.006. Epub 2020 Jul 19. Aust Crit Care. 2021. PMID: 32698985
-
Wrist actigraphy.Chest. 2011 Jun;139(6):1514-1527. doi: 10.1378/chest.10-1872. Chest. 2011. PMID: 21652563 Free PMC article. Review.
Cited by
-
Sleeping for two: a cross-sectional study on associations between objectively measured sleep during early to mid-pregnancy and maternal and fetal outcomes and inflammatory biomarker profiles.BMC Pregnancy Childbirth. 2025 May 5;25(1):533. doi: 10.1186/s12884-025-07634-9. BMC Pregnancy Childbirth. 2025. PMID: 40325393 Free PMC article.
-
Poor agreement between actigraphy and polysomnography for assessing sleep during post-traumatic amnesia.J Clin Sleep Med. 2023 Jan 1;19(1):201. doi: 10.5664/jcsm.10318. J Clin Sleep Med. 2023. PMID: 36123950 Free PMC article. No abstract available.
-
Sleep assessment during early amnesic brain injury recovery.J Clin Sleep Med. 2023 Jan 1;19(1):203-204. doi: 10.5664/jcsm.10326. J Clin Sleep Med. 2023. PMID: 36239050 Free PMC article. No abstract available.
-
Unfolding the role of exercise in the management of sleep disorders.Eur J Appl Physiol. 2024 Sep;124(9):2547-2560. doi: 10.1007/s00421-024-05556-6. Epub 2024 Jul 20. Eur J Appl Physiol. 2024. PMID: 39031176 Free PMC article. Review.
References
-
- Fedele B , McKenzie D , Williams G , Giles R , Olver J . Assessing sleep architecture with polysomnography during posttraumatic amnesia after traumatic brain injury: a pilot study . Neurorehabil Neural Repair. 2021. ; 35 ( 7 ): 622 – 633 . - PubMed
-
- Makley MJ , Johnson-Greene L , Tarwater PM , et al. . Return of memory and sleep efficiency following moderate to severe closed head injury . Neurorehabil Neural Repair. 2009. ; 23 ( 4 ): 320 – 326 . - PubMed
-
- Fedele B , Williams G , McKenzie D , Sutherland E , Olver J . Subacute sleep disturbance in moderate to severe traumatic brain injury: a systematic review . Brain Inj. 2020. ; 34 ( 3 ): 316 – 327 . - PubMed
-
- Ouellet MC , Beaulieu-Bonneau S , Morin CM . Sleep-wake disturbances after traumatic brain injury . Lancet Neurol. 2015. ; 14 ( 7 ): 746 – 757 . - PubMed
-
- Ponsford J , Janzen S , McIntyre A , Bayley M , Velikonja D , Tate R ; INCOG Expert Panel . INCOG recommendations for management of cognition following traumatic brain injury, part I: posttraumatic amnesia/delirium . J Head Trauma Rehabil. 2014. ; 29 ( 4 ): 307 – 320 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
