

Neuroprotection against ischemic stroke requires a specific class of early responder T cells in mice
- PMID: 35912857
- PMCID: PMC9337834
- DOI: 10.1172/JCI157678
Neuroprotection against ischemic stroke requires a specific class of early responder T cells in mice
Abstract
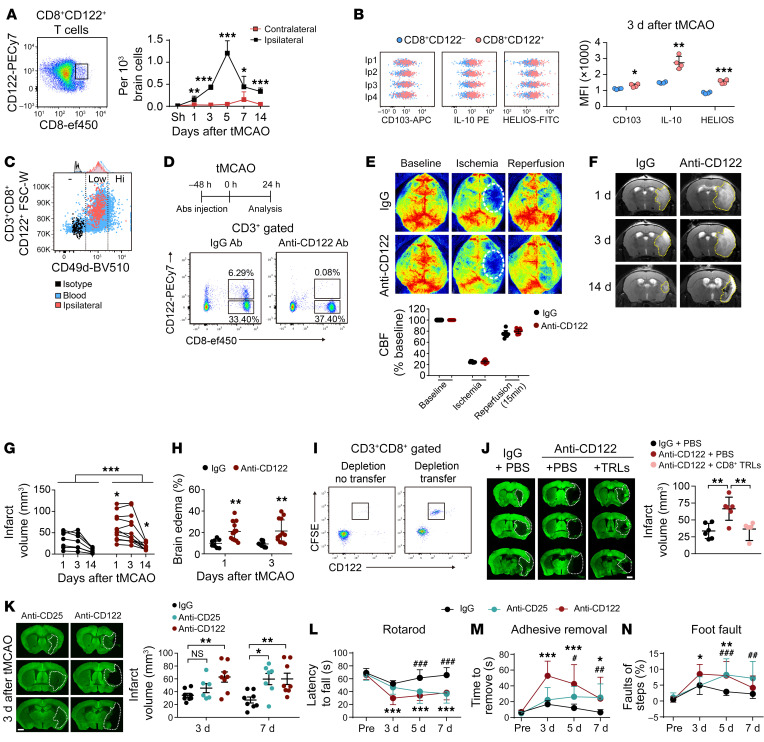
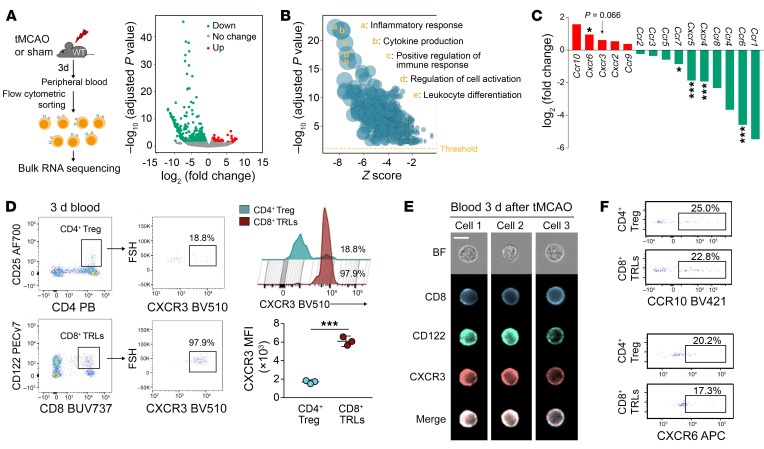
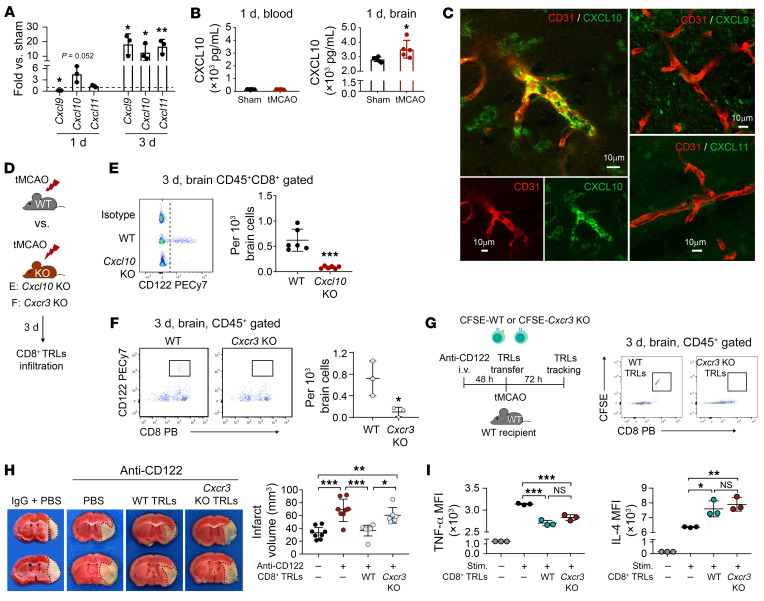
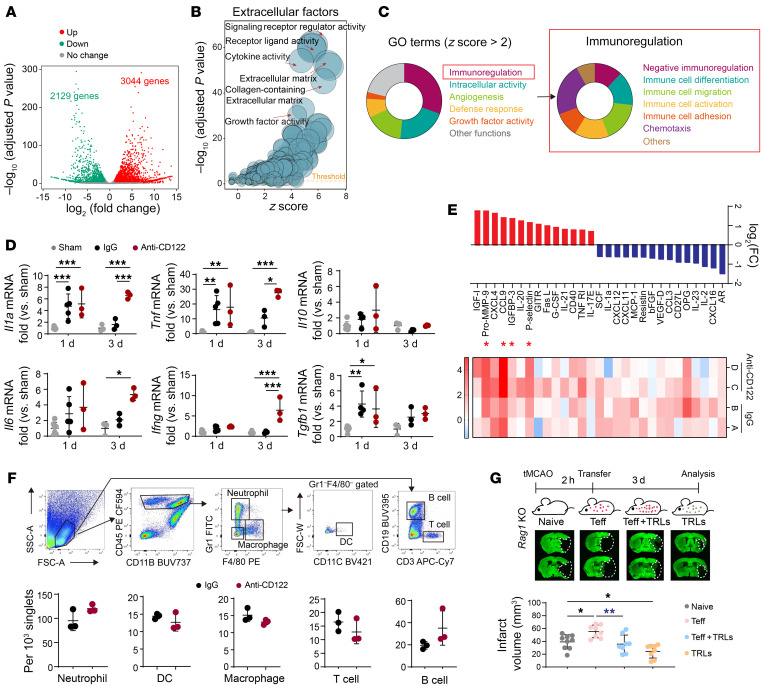
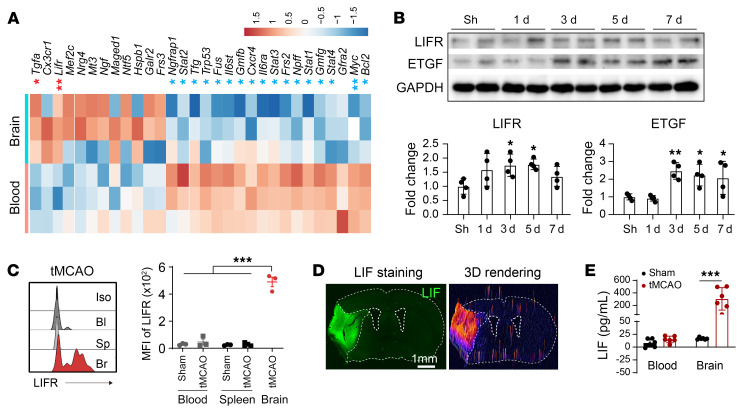
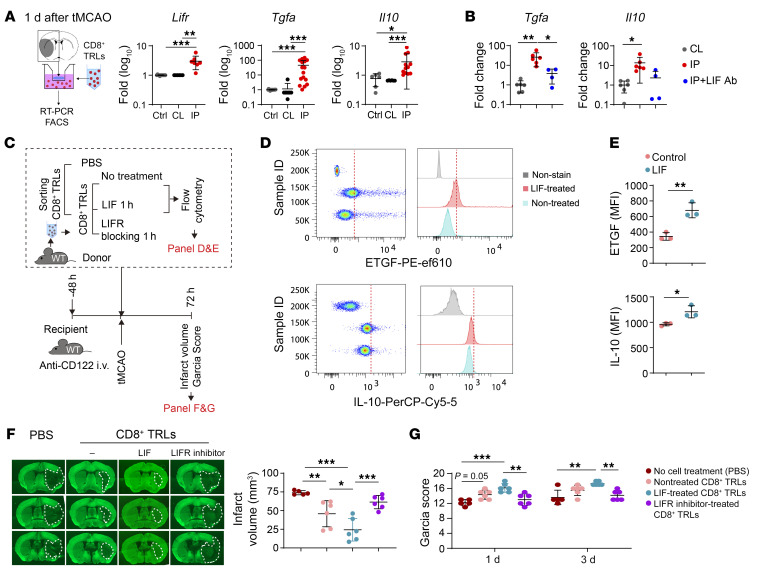
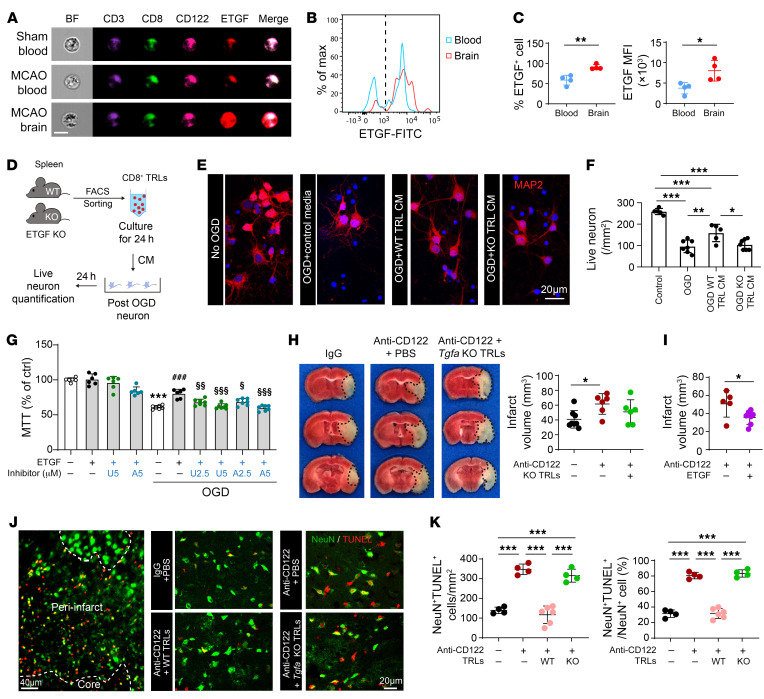
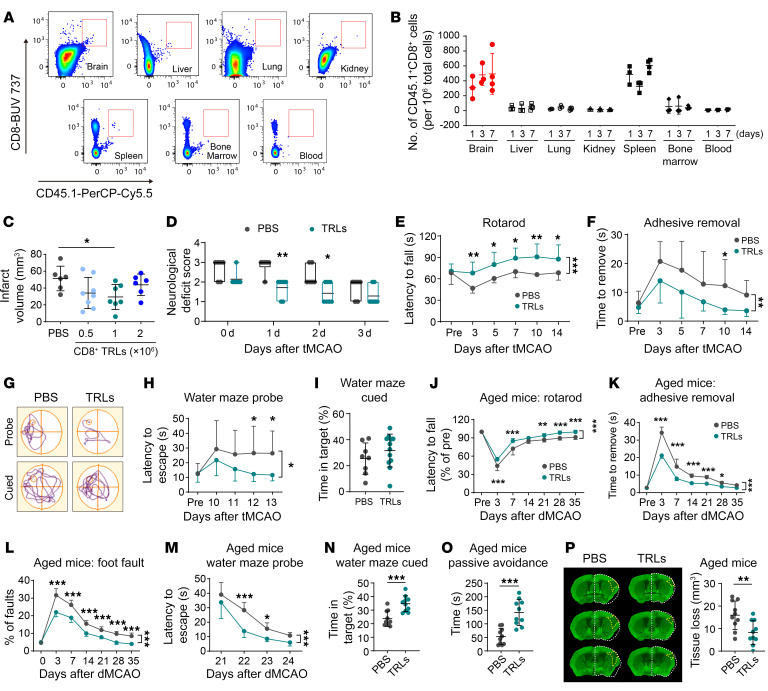
Immunomodulation holds therapeutic promise against brain injuries, but leveraging this approach requires a precise understanding of mechanisms. We report that CD8+CD122+CD49dlo T regulatory-like cells (CD8+ TRLs) are among the earliest lymphocytes to infiltrate mouse brains after ischemic stroke and temper inflammation; they also confer neuroprotection. TRL depletion worsened stroke outcomes, an effect reversed by CD8+ TRL reconstitution. The CXCR3/CXCL10 axis served as the brain-homing mechanism for CD8+ TRLs. Upon brain entry, CD8+ TRLs were reprogrammed to upregulate leukemia inhibitory factor (LIF) receptor, epidermal growth factor-like transforming growth factor (ETGF), and interleukin 10 (IL-10). LIF/LIF receptor interactions induced ETGF and IL-10 production in CD8+ TRLs. While IL-10 induction was important for the antiinflammatory effects of CD8+ TRLs, ETGF provided direct neuroprotection. Poststroke intravenous transfer of CD8+ TRLs reduced infarction, promoting long-term neurological recovery in young males or aged mice of both sexes. Thus, these unique CD8+ TRLs serve as early responders to rally defenses against stroke, offering fresh perspectives for clinical translation.
Keywords: Immunotherapy; Inflammation; Neuroscience; Stroke; T cells.
Figures
Comment in
-
Revisiting regulatory T cells for stroke therapy.J Clin Invest. 2022 Aug 1;132(15):e161703. doi: 10.1172/JCI161703. J Clin Invest. 2022. PMID: 35912860 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
