

Coffee and tea consumption, patient-reported, and clinical outcomes in a longitudinal study of patients with breast cancer
- PMID: 35913436
- PMCID: PMC9541449
- DOI: 10.1002/cncr.34401
Coffee and tea consumption, patient-reported, and clinical outcomes in a longitudinal study of patients with breast cancer
Abstract
Background: Higher consumption of coffee and tea has been associated with improved health outcomes in the general population and improved breast cancer (BC) prognosis. This study investigated patterns of coffee and tea consumption and association with patient-reported outcomes (PROs) and clinical outcomes among survivors of BC.
Methods: The authors included survivors of stage I-III BC enrolled in the CANTO cohort (NCT01993498) that provided post-treatment assessment of coffee and tea consumption from years 1 to 4 after diagnosis. Group-based trajectory modeling clustered patients according to daily consumption of coffee and tea. Multivariable mixed models and Cox models examined associations between consumption, PROs and clinical outcomes.
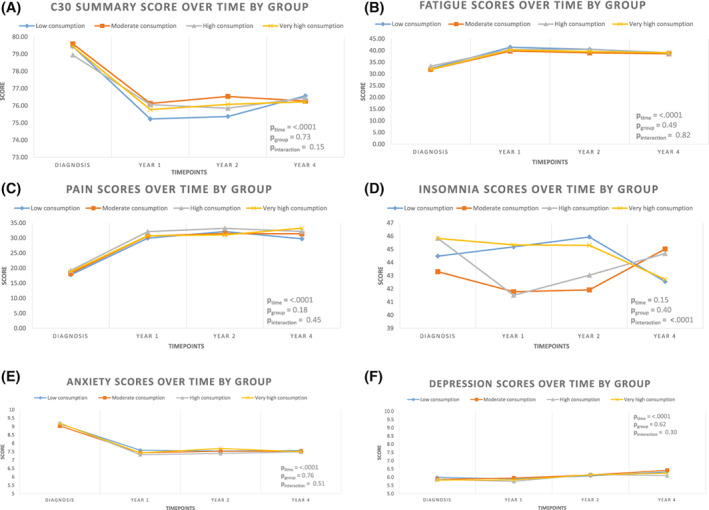
Results: Among 3788 patients, the authors identified four stable patterns of consumption: "Low" (25.8%), "Moderate" (37.6%), "High" (25.3%), and "Very high" (11.3%), corresponding to <1, 2, 3, and ≥ 4 cups of coffee and/or tea per day. Patients in the "Very high" group (vs. "Low"), were more likely to be younger, smokers, with higher monthly income and education. PROs and survival outcomes were similar across the four groups.
Conclusions: Over one in three survivors of BC reported high or very high consumption of coffee and/or tea. The authors found no association between higher consumption of coffee and/or tea, worse PROs and clinical outcomes.
Keywords: breast cancer; coffee; patient-reported outcome measures; survivors; tea.
© 2022 The Authors. Cancer published by Wiley Periodicals LLC on behalf of American Cancer Society.
Conflict of interest statement
Ines Vaz‐Luis reports honoraria from Amgen, Pfizer, Novartis, and AstraZeneca. Barbara Pistilli reports consulting/advising for Puma Biotechnology, Novartis, Myriad Genetics, and Pierre Fabre; meeting or travel support from Novartis, AstraZeneca, MSD Oncology, and Pfizer; and research funding from Daiichi, Puma Biotechnology, Novartis, Merus, AstraZeneca, Pfizer and AstraZeneca. Fabrice André reports research funding from Novartis, Pfizer, AstraZeneca, Eli Lilly, Daichii, and Roche. Paul Cottu reports funding from Pfizer and Nanostring; consulting fees from Pfizer, Roche, Lilly, Novartis, Daichi, and Seagen; payment for lecture presentations from Pfizer; and payment for manuscript writing from Novartis. Lucia Del Mastro reports grants or contracts from Eli Lilly, Novartis, Roche, Daiichi Sankyo, and Seagan; payment or honoraria from Roche, Novartis, Pfizer, Eli Lilly, AstraZeneca, MSD, Seagen, Gilead, Pierre Fabre, Eisai, Exact Sciences, and Ipsen; support for attending meetings or travel from Roche, Pfizer, and Eisai; and participation on a Data Safety Monitoring Board or Advisory Board from Novartis, Roche, Eli Lilly, Pfizer, Daiichi Sakyo, Exact Sciences, Gilead, Pierre Fabre, Eisai, and AstraZeneca. Olivier Tredan reports payment or honoraria from Roche, Pfizer, Novartis‐Sandoz, Lilly, MSD, Astra‐Zeneca, Pierre Fabre, Seagen, Daiichi‐Sankyo, Gilead, and Eisai; support for attending meetings and/or travel from Roche, Pfizer, Novartis‐Sandoz, Lilly, MSD, Astra‐Zeneca, Pierre Fabre, Seagen, Daiichi‐Sankyo, Gilead, and Eisai; and support for Participation on a Data Safety Monitoring Board or Advisory Board from Roche, Pfizer, Novartis‐Sandoz, Lilly, MSD, Astra‐Zeneca, Pierre Fabre, Seagen, Daiichi‐Sankyo, Gilead, and Eisai.
Figures
Similar articles
-
Prospective study of breast cancer in relation to coffee, tea and caffeine in Sweden.Int J Cancer. 2015 Oct 15;137(8):1979-89. doi: 10.1002/ijc.29569. Epub 2015 Apr 30. Int J Cancer. 2015. PMID: 25885188
-
Coffee and tea intake and risk of breast cancer.Breast Cancer Res Treat. 2010 Jun;121(2):461-7. doi: 10.1007/s10549-009-0583-y. Epub 2009 Oct 22. Breast Cancer Res Treat. 2010. PMID: 19847643
-
Post-diagnostic coffee and tea consumption and breast cancer survival.Br J Cancer. 2021 May;124(11):1873-1881. doi: 10.1038/s41416-021-01277-1. Epub 2021 Mar 24. Br J Cancer. 2021. PMID: 33762714 Free PMC article.
-
Coffee and tea consumption in relation to the risk of large bowel cancer: a review of epidemiologic studies.Cancer Lett. 1990 Jul 31;52(3):163-71. doi: 10.1016/0304-3835(90)90183-x. Cancer Lett. 1990. PMID: 2199027 Review.
-
Are coffee and tea consumption associated with urinary tract cancer risk? A systematic review and meta-analysis.Int J Epidemiol. 2001 Apr;30(2):353-62. doi: 10.1093/ije/30.2.353. Int J Epidemiol. 2001. PMID: 11369742
Cited by
-
Coffee and tea intake and survival of cancer patients: a systematic review and meta-analysis.Cancer Causes Control. 2025 Jul 11. doi: 10.1007/s10552-025-02033-z. Online ahead of print. Cancer Causes Control. 2025. PMID: 40643840
-
Health Benefits of Coffee Consumption for Cancer and Other Diseases and Mechanisms of Action.Int J Mol Sci. 2023 Jan 31;24(3):2706. doi: 10.3390/ijms24032706. Int J Mol Sci. 2023. PMID: 36769029 Free PMC article. Review.
-
The Chemopreventive Effects of Chlorogenic Acids, Phenolic Compounds in Coffee, against Inflammation, Cancer, and Neurological Diseases.Molecules. 2023 Mar 4;28(5):2381. doi: 10.3390/molecules28052381. Molecules. 2023. PMID: 36903626 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
