

Mental health and periodontal and peri-implant diseases
- PMID: 35913583
- PMCID: PMC9804456
- DOI: 10.1111/prd.12452
Mental health and periodontal and peri-implant diseases
Abstract
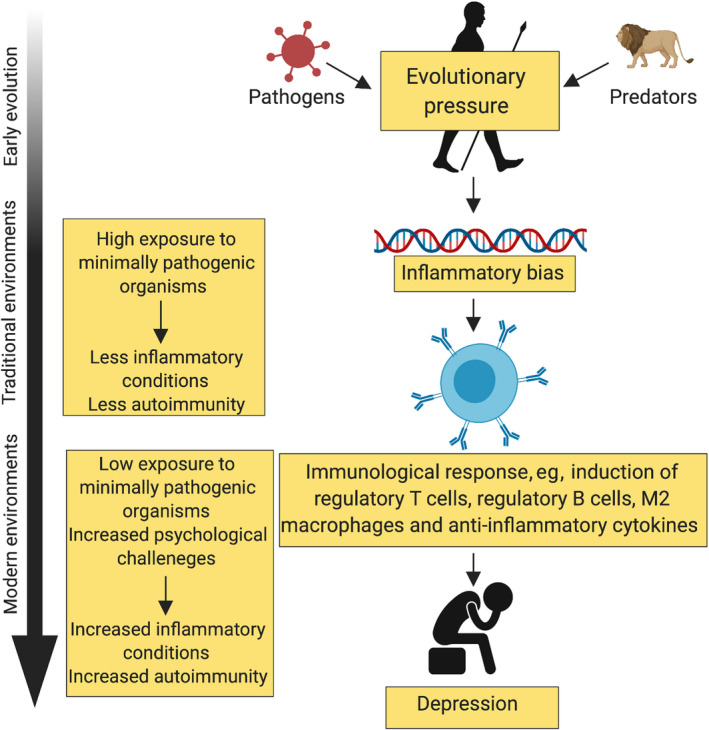
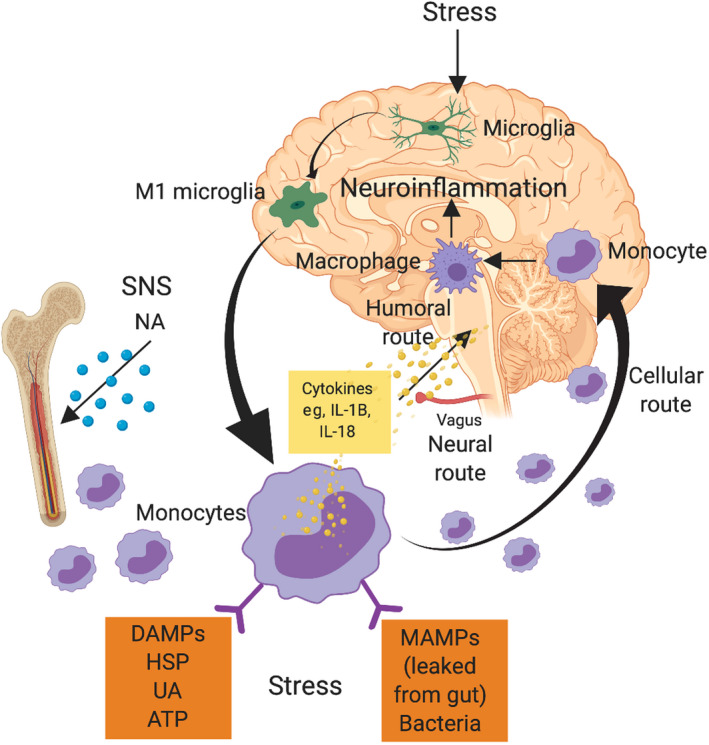
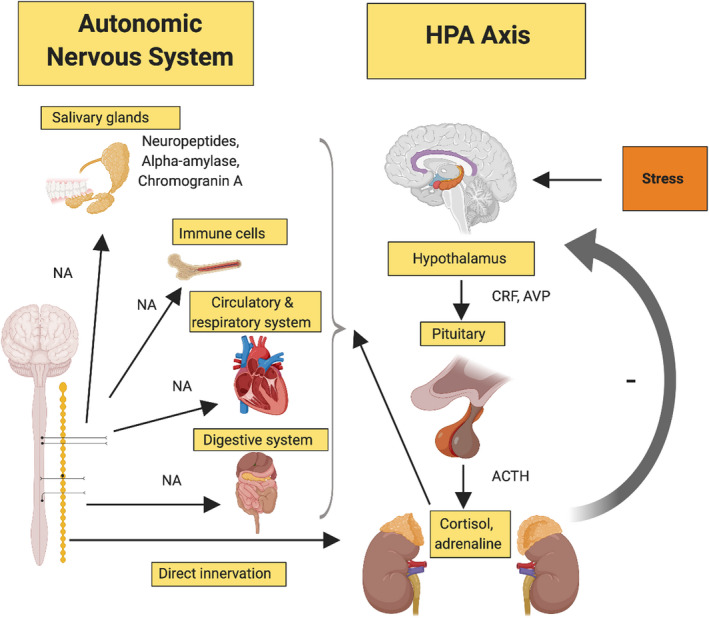
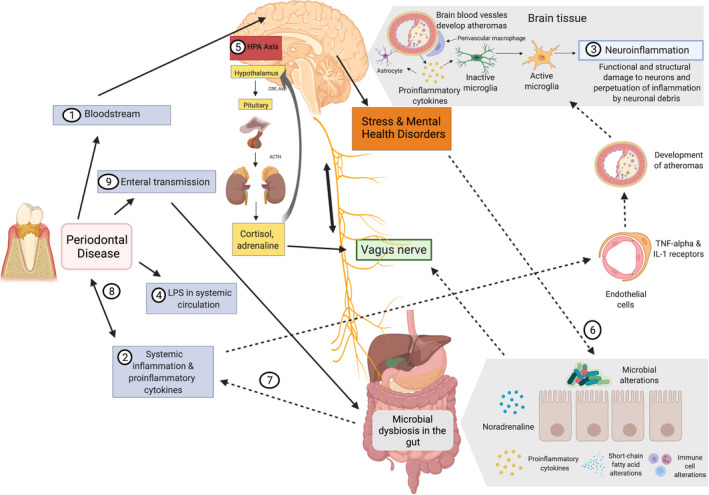
Mental health disorders, particularly depression and anxiety, affect a significant number of the global population. Several pathophysiological pathways for these disorders have been identified, including the hypothalamic-pituitary-adrenal axis, autonomic nervous system, and the immune system. In addition, life events, environmental factors, and lifestyle affect the onset, progression, and recurrence of mental health disorders. These may all overlap with periodontal and/or peri-implant disease. Mental health disorders are associated with more severe periodontal disease and, in some cases, poorer healing outcomes to nonsurgical periodontal therapy. They can result in behavior modification, such as poor oral hygiene practices, tobacco smoking, and alcohol abuse, which are also risk factors for periodontal disease and, therefore, may have a contributory effect. Stress has immunomodulatory effects regulating immune cell numbers and function, as well as proinflammatory cytokine production. Stress markers such as cortisol and catecholamines may modulate periodontal bacterial growth and the expression of virulence factors. Stress and some mental health disorders are accompanied by a low-grade chronic inflammation that may be involved in their relationship with periodontal disease and vice versa. Although the gut microbiome interacting with the central nervous system (gut-brain axis) is thought to play a significant role in mental illness, less is understood about the role of the oral microbiome. The evidence for mental health disorders on implant outcomes is lacking, but may mainly be through behaviourial changes. Through lack of compliance withoral hygiene and maintenance visits, peri-implant health can be affected. Increased smoking and risk of periodontal disease may also affect implant outcomes. Selective serotonin reuptake inhibitors have been linked with higher implant failure. They have an anabolic effect on bone, reducing turnover, which could account for the increased loss.
Keywords: Alzheimer disease; anxiety disorder; bipolar; depression; gut-brain axis; mental health; microbiome; mood (affective) disorder; peri-implant disease; periodontal disease; schizophrenia; stress; substance use disorder.
© 2022 The Authors. Periodontology 2000 published by John Wiley & Sons Ltd.
Figures

References
-
- American Academy of Periodontology . American Academy of Periodontology Task Force report on the update to the 1999 classification of periodontal diseases and conditions. J Periodontol. 2015;86(7):835‐838. - PubMed
-
- Lang NP, Berglundh T, Working Group 4 of Seventh European Workshop on Periodontology . Periimplant diseases: where are we now?–Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011;38 (suppl 11):178‐181. - PubMed
-
- Lindhe J, Meyle J, Group D of European Workshop on Periodontology . Peri‐implant diseases: consensus report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008;35(8 suppl):282‐285. - PubMed
-
- Albandar JM, Rams TE. Global epidemiology of periodontal diseases: an overview. Periodontol 2000. 2002;29(1):7‐10. - PubMed
-
- Eke PI, Dye B, Wei L, Thornton‐Evans G, Genco R. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J Dent Res. 2012;91(10):914‐920. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
