

Intracranially Extended Sinonasal Undifferentiated Carcinoma: A Case Report and Literature Review
- PMID: 35913898
- PMCID: PMC9353759
- DOI: 10.12659/AJCR.935876
Intracranially Extended Sinonasal Undifferentiated Carcinoma: A Case Report and Literature Review
Abstract
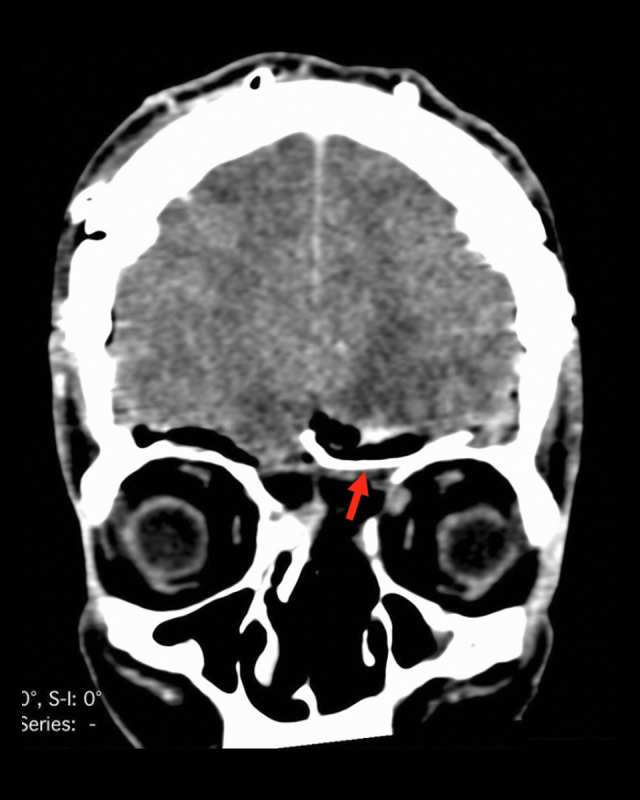
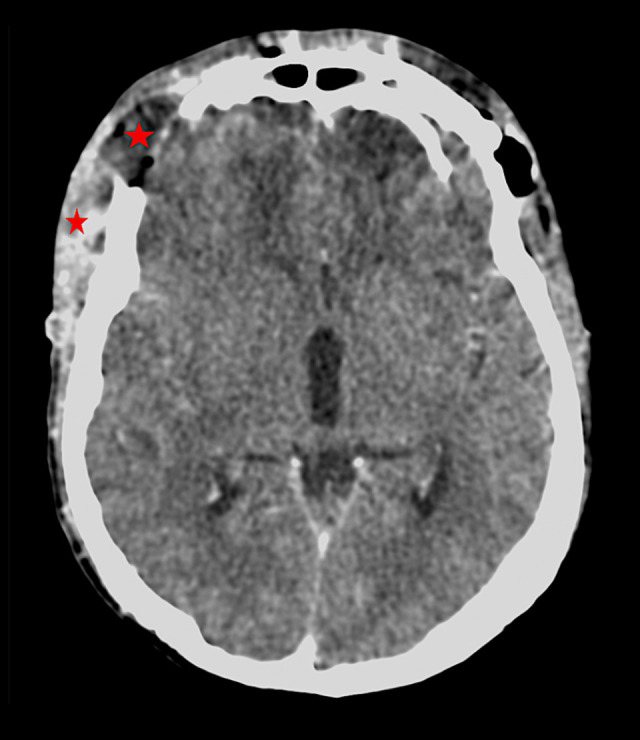
BACKGROUND Sinonasal undifferentiated carcinomas (SNUC) are highly malignant and rare lesions. Therapeutic efforts often provide frustrating results. Their course is characterized by indolent progression, until it culminates in extensive local infiltration of adjacent anatomical structures or cervical lymphadenopathy in approximately one-third of patients upon admission. It most frequently affects males, with a sex ratio of 3: 1. The age at manifestation tends to be about 40-50 years. CASE REPORT We report the case of a 41-year-old man with intracranial expansion of SNUC. Two previous sinus surgeries were performed endoscopically because the lesion at that moment was exclusively located endonasally. Within the last few months, he had been having persistent headaches. Magnetic resonance imaging (MRI) revealed an anterior cranial fossa lesion. Therefore, he underwent a bifrontal craniotomy and excision of the space-occupying lesion (SOL). The osseous defect of the skull base was covered with a titanium mesh. Finally, we performed a duraplasty using a pericranial flap and fat tissue taken from his abdomen. Postoperatively, his wound was dehisced. We proceeded then to a frontal craniectomy with surgical debridement, subgaleal empyem and epidural abscess removal, and copious irrigation with oxygen peroxide. Enterococcus spp. were isolated from pus cultures. Despite receiving bacteria-focused antibiotics, he unfortunately developed sepsis and died. The histopathologic findings revealed a SNUC, which is the criterion standard for diagnosis. CONCLUSIONS Multimodal treatment offers the best prognosis to patients with SNUC. Combined operations by otolaryngologists and neurosurgeons provide the necessary radicality. There is high risk of wound healing disorders, especially when local irradiation had been administered.
Conflict of interest statement
Figures



Similar articles
-
Leptomeningeal carcinomatosis in sinonasal undifferentiated carcinoma.Head Neck. 2013 Nov;35(11):E343-5. doi: 10.1002/hed.23225. Epub 2013 Mar 8. Head Neck. 2013. PMID: 23471826
-
Sinonasal undifferentiated carcinoma with metastasis to the extradural spine.Br J Neurosurg. 2023 Aug;37(4):627-629. doi: 10.1080/02688697.2018.1529297. Epub 2018 Nov 19. Br J Neurosurg. 2023. PMID: 30450992
-
Sinonasal undifferentiated carcinoma: case series and review of the literature.Neurosurgery. 2000 Sep;47(3):750-4; discussion 754-5. doi: 10.1097/00006123-200009000-00045. Neurosurgery. 2000. PMID: 10981763 Review.
-
Sinonasal Undifferentiated Carcinoma.Curr Oncol Rep. 2019 Feb 26;21(3):26. doi: 10.1007/s11912-019-0776-4. Curr Oncol Rep. 2019. PMID: 30806835 Review.
-
Minimally invasive endoscopic resection of sinonasal undifferentiated carcinoma.Am J Otolaryngol. 2011 Nov-Dec;32(6):464-9. doi: 10.1016/j.amjoto.2010.09.006. Epub 2010 Oct 30. Am J Otolaryngol. 2011. PMID: 21041001
References
-
- Frierson HF, Jr, Mills SE, Fechner RE, et al. Sinonasal undifferentiated carcinoma. An aggressive neoplasm derived from Schneiderian epithelium and distinct from olfactory neuroblastoma. Am J Surg Pathol. 1986;10(11):771–79. - PubMed
-
- Reiersen DA, Pahilan ME, Devaiah AK. Meta-analysis of treatment outcomes for sinonasal undifferentiated carcinoma. Otolaryngol Head Neck Surg. 2012;147(1):7–14. - PubMed
-
- Rischin D, Porceddu S, Peters L, et al. Promising results with chemoradiation in patients with sinonasal undifferentiated carcinoma. Head Neck. 2004;26(5):435–41. - PubMed
-
- Mills SE. Neuroendocrine tumors of the head and neck: A selected review with emphasis on terminology. Endocr Pathol. 1996;7(4):329–43. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Miscellaneous
