

Automated Detection of Speech Timing Alterations in Autopsy-Confirmed Nonfluent/Agrammatic Variant Primary Progressive Aphasia
- PMID: 35914945
- PMCID: PMC9421598
- DOI: 10.1212/WNL.0000000000200750
Automated Detection of Speech Timing Alterations in Autopsy-Confirmed Nonfluent/Agrammatic Variant Primary Progressive Aphasia
Abstract
Background and objectives: Motor speech function, including speech timing, is a key domain for diagnosing nonfluent/agrammatic variant primary progressive aphasia (nfvPPA). Yet, standard assessments use subjective, specialist-dependent evaluations, undermining reliability and scalability. Moreover, few studies have examined relevant anatomo-clinical alterations in patients with pathologically confirmed diagnoses. This study overcomes such caveats using automated speech timing analyses in a unique cohort of autopsy-proven cases.
Methods: In a cross-sectional study, we administered an overt reading task and quantified articulation rate, mean syllable and pause duration, and syllable and pause duration variability. Neuroanatomical disruptions were assessed using cortical thickness and white matter (WM) atrophy analysis.
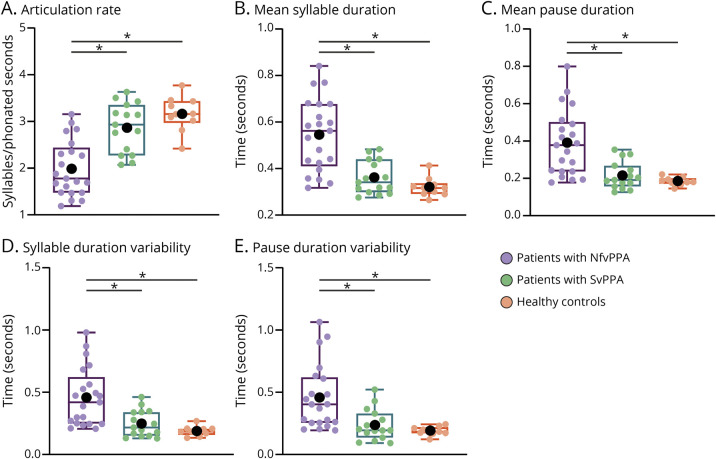
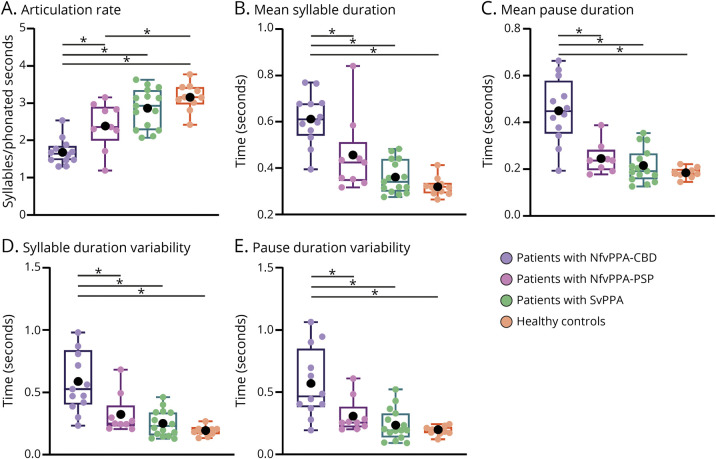
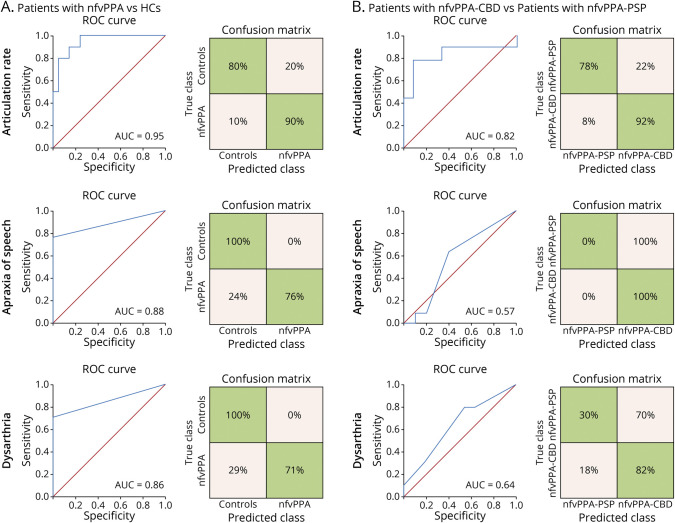
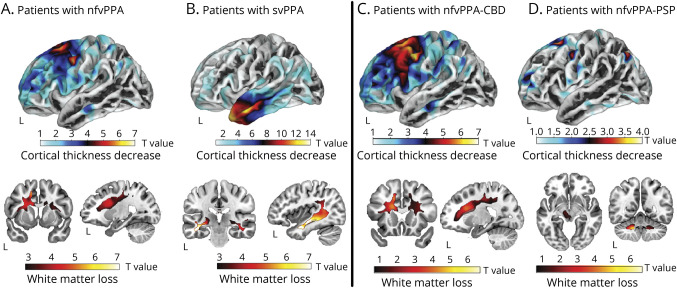
Results: We evaluated 22 persons with nfvPPA (mean age: 67.3 years; 13 female patients) and confirmed underlying 4-repeat tauopathy, 15 persons with semantic variant primary progressive aphasia (svPPA; mean age: 66.5 years; 8 female patients), and 10 healthy controls (HCs; 70 years; 5 female patients). All 5 speech timing measures revealed alterations in persons with nfvPPA relative to both the HC and svPPA groups, controlling for dementia severity. The articulation rate robustly discriminated individuals with nfvPPA from HCs (area under the ROC curve [AUC] = 0.95), outperforming specialist-dependent perceptual measures of dysarthria and apraxia of speech severity. Patients with nfvPPA exhibited structural abnormalities in left precentral and middle frontal as well as bilateral superior frontal regions, including their underlying WM. The articulation rate correlated with atrophy of the left pars opercularis and supplementary/presupplementary motor areas. Secondary analyses showed that, controlling for dementia severity, all measures yielded greater deficits in patients with nfvPPA and corticobasal degeneration (nfvPPA-CBD, n = 12) than in those with progressive supranuclear palsy pathology (nfvPPA-PSP, n = 10). The articulation rate robustly discriminated between individuals in each subgroup (AUC = 0.82). More widespread cortical thinning was observed for the nfvPPA-CBD than the nfvPPA-PSP group across frontal regions.
Discussion: Automated speech timing analyses can capture specific markers of nfvPPA while potentially discriminating between patients with different tauopathies. Thanks to its objectivity and scalability; this approach could support standard speech assessments.
Classification of evidence: This study provides Class III evidence that automated speech analysis can accurately differentiate patients with nonfluent PPA from normal controls and patients with semantic variant PPA.
© 2022 American Academy of Neurology.
Figures
Comment in
-
Advances and Remaining Challenges in Distinguishing Variants of Primary Progressive Aphasia.Neurology. 2022 Aug 2;99(5):181-182. doi: 10.1212/WNL.0000000000200864. Neurology. 2022. PMID: 35914943 No abstract available.
References
-
- Josephs KA, Duffy JR. Apraxia of speech and nonfluent aphasia: a new clinical marker for corticobasal degeneration and progressive supranuclear palsy. Curr Opin Neurol. 2008;21(6):688-692. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous