

[Proximal femoral varus osteotomy in Legg-Calve-Perthes disease]
- PMID: 35915149
- PMCID: PMC9525383
- DOI: 10.1007/s00064-022-00778-3
[Proximal femoral varus osteotomy in Legg-Calve-Perthes disease]
Abstract
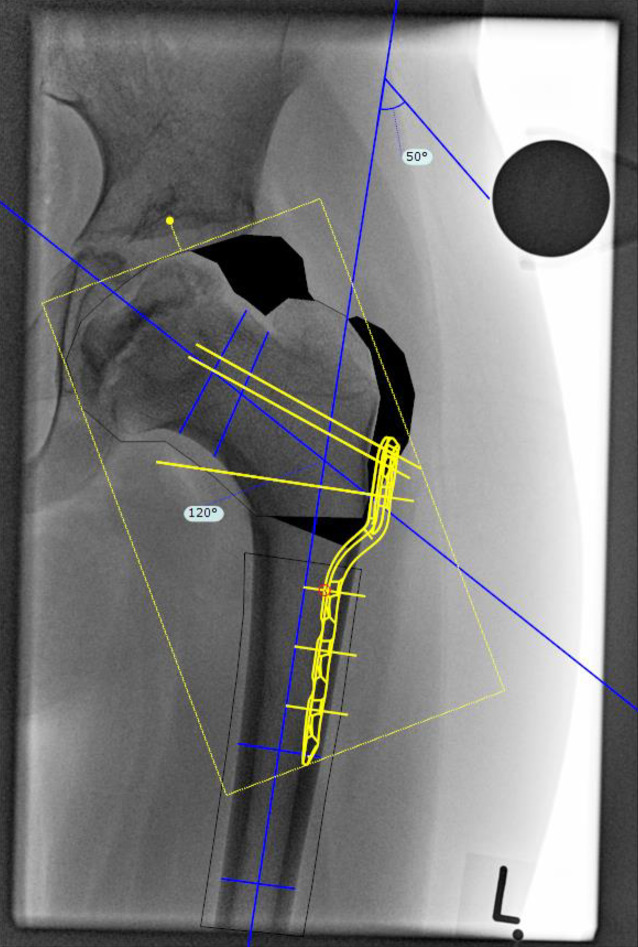
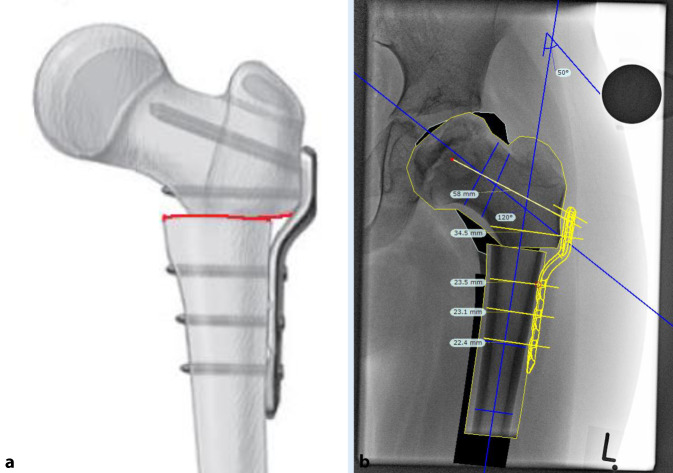
Objective: The proximal femoral varus osteotomy (FVO) aims to re-centre the femoral head in the acetabular socket after prognostically unfavourable subluxation, e.g. in Legg-Calve-Perthes disease (LCPD).
Indications: No unified indication criteria have been defined yet for containment therapy in LCPD. However, specific radiographic features related to deformity development, age at diagnosis or onset and classifications describing pathomorphological changes in the femoral head related to bone necrosis can support decisionmaking.
Contraindications: Absolute contraindications-a hinge abducted joint; failure of femoral head reduction in the 20° abduction anteroposterior view; total epiphyseal necrosis. Relative contraindication-children < 6 years, in lateral pillar classification group A or Catteral group I and II.
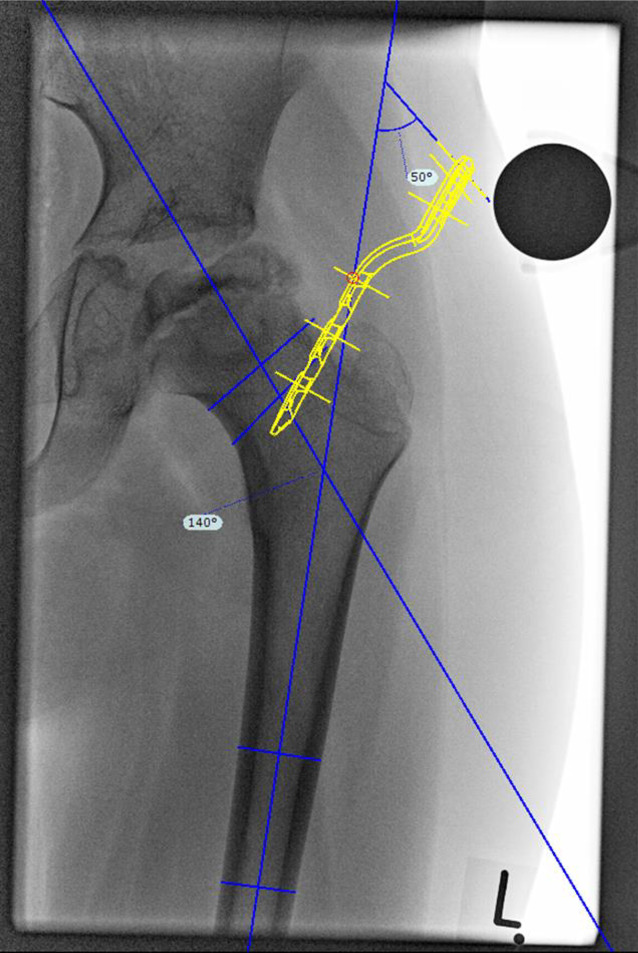
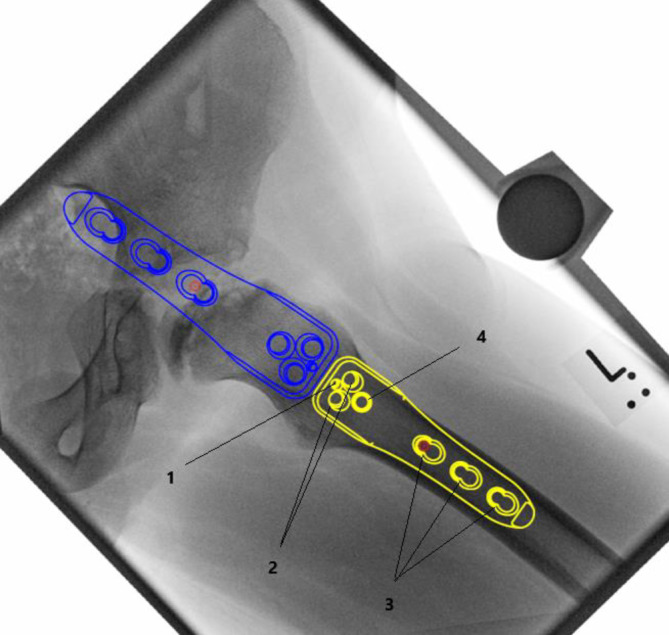
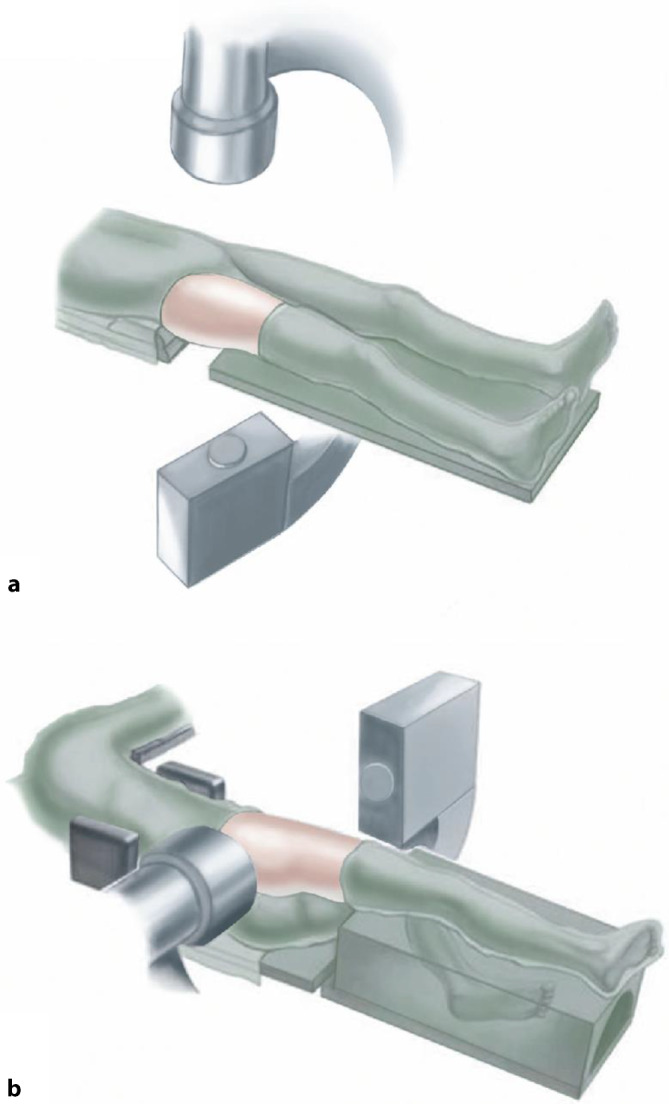
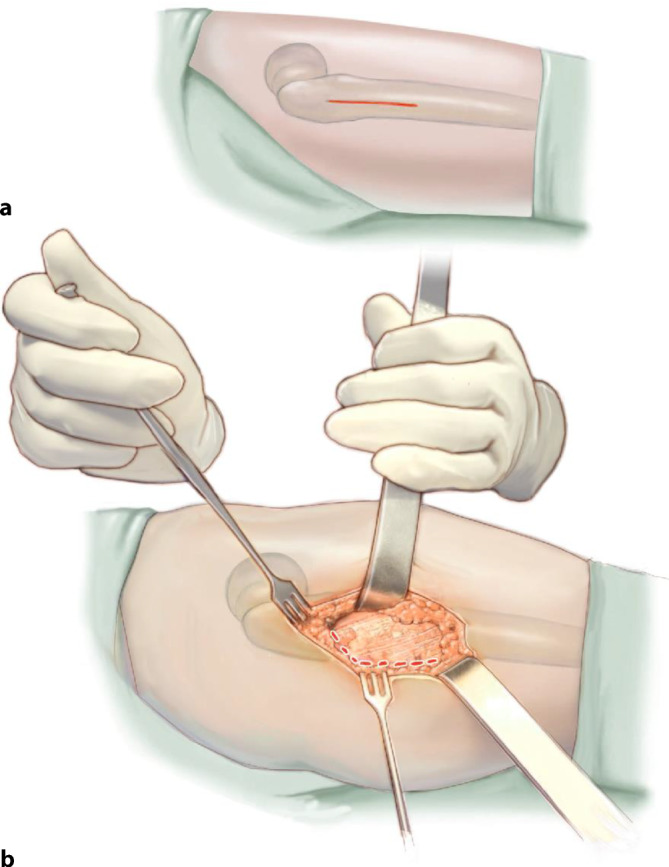
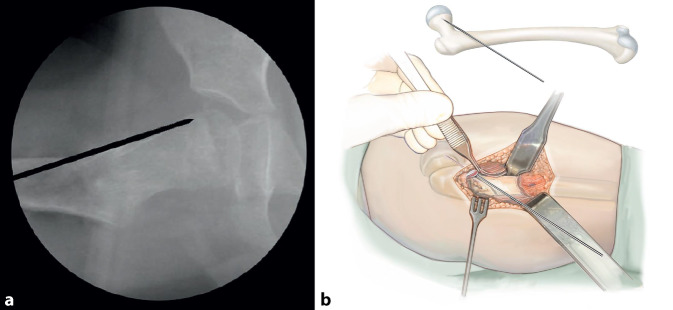
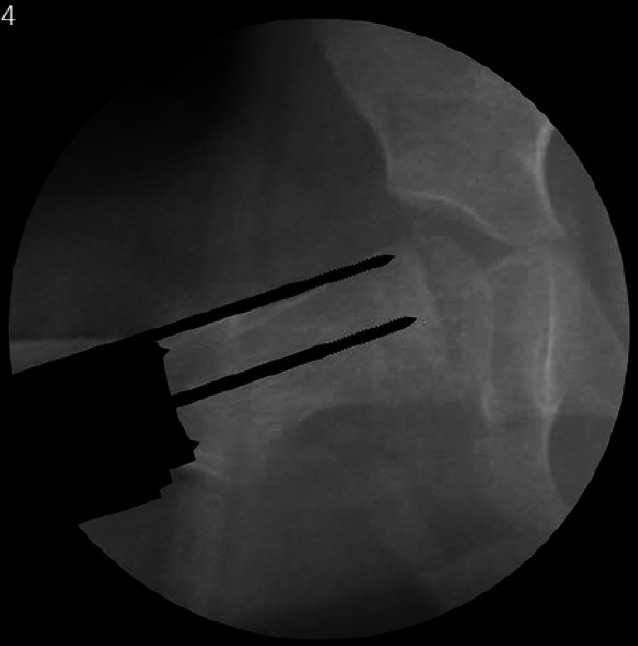
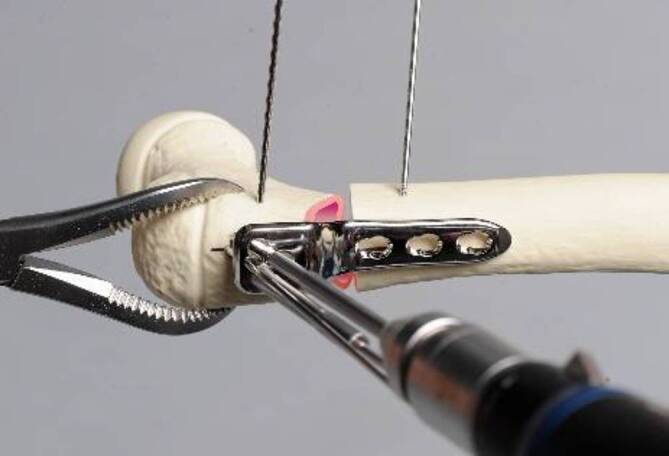
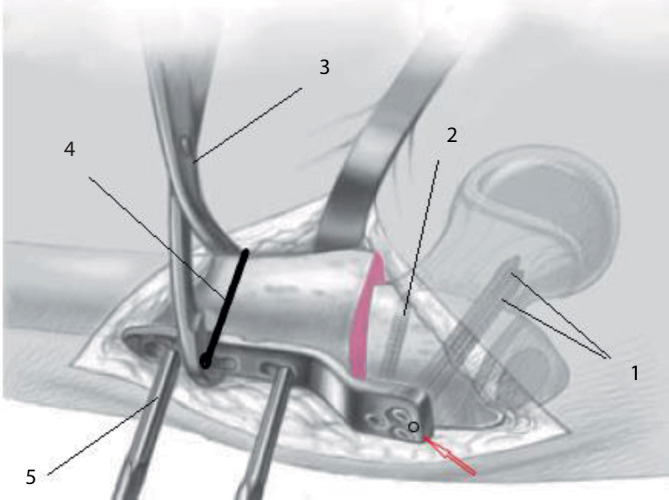
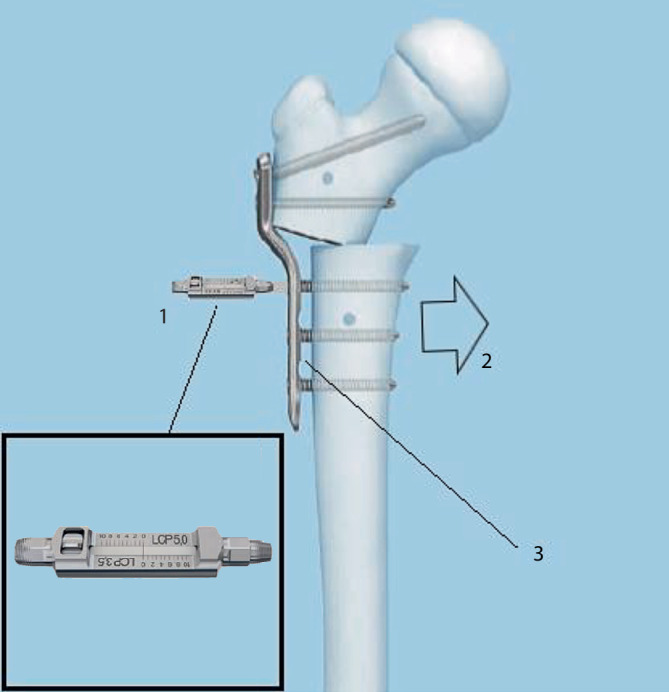
Surgical technique: Lateral approach to the proximal femur. Insertion of the first K‑wire to mark the anteversion of the femoral neck. Additional K‑wires are placed parallel to the first via the positioner aiming block. Lokalise the optimal postion for the osteotomy. Insertion of additional K‑wires in the distal fragment an facilitate manipulation and serve as reference for derotation. After osteotomy proximal fixation of the plate with locking screws replacing the K-wires. Insertion of a cortical screw into the middle hole to achieve optimal interfragmentary compression. Remaining locking screws are inserted and cortical screw replaced by a locking screw.
Postoperative management: Mobilization with heel-touch weight-bearing on crutches for 6 weeks. Increased weightbearing after radiographic follow-up as soon as sufficient bone union is present. Implant removal after 9-12 months. Return to sports after 3 months.
Results: The FVO has been used in the surgical treatment of severe LCPD for nearly 60 years and is established worldwide. Growing knowledge and consecutive optimization of the surgery indication together with the new implants contribute to improving clinical and radiological outcomes and reducing intraoperative and postoperative complications.
Zusammenfassung: OPERATIONSZIEL: Die proximale femorale Varisationsosteotomie (PVO) ist eine chirurgische Technik zur Rezentrierung des Hüftkopfes, sofern es bspw. im Rahmen der ablaufenden Legg-Calvé-Perthes(LCPD)-Krankheit zur Subluxation gekommen ist.
Indikationen: Bis anhin existieren keine einheitlichen Indikationskriterien für die Containment-Therapie bei LCPD-Patienten. Einzelne, für die Deformitätsentwicklung prädiktive radiologische Faktoren, Alter bei Diagnosestellung oder Symptombeginn und Klassifikationen, welche die Pathomorphologie des Femurkopfes bezogen auf die Nekrose beschreiben, können die Indikationsstellung erleichtern.
Kontraindikationen: Die absolute Kontraindikation stellt die Entwicklung eines Scharniergelenkes dar (Hinge-Abduktion). Bleibt der Femurkopf in einer Abduktionsröntgenaufnahme von 20° auch in Abwesenheit einer Hinge-Abduktion dezentriert oder besteht ein Total-Kopf-Befall, ergibt sich ebenfalls eine Kontraindikation. Relativ kontraindiziert ist die PVO bei Kindern mit Beginn der Erkrankung < 6 Jahren, in der Lateral-Pillar-Klassifikation Gruppe A soiwe bei I und II nach Catterall.
Operationstechnik: Lateraler Standardzugang zum proximalen Femur. Platzieren des Anteversions-K-Drahtes ventral des Schenkelhalses. Weitere K-Drähte werden parallel mithilfe von Positionierinstrumenten in den Schenkelhals eingebracht. Der optimale Bereich für die Osteotomie wird aufgesucht. Für die Vereinfachung der Manipulation des distalen Fragments und als Referenz für die Derotation werden am Femurschaft weitere K‑Drähte eingebracht. Nach Femurosteotomie erfolgt proximales Fixieren der Platte durch sukzessives Auswechseln der K‑Drähte gegen winkelstabile Schrauben. Die interfragmentäre Kompression erzeugt eine exzentrisch positionierte Kortikalisschraube im mittleren distalen Plattenloch. Die weitere distale Fixation der Platte erfolgt mit winkelstabilen Schrauben. Auswechseln der Kortikalisschraube gegen eine weitere winkelstabile Schraube. Alternativ zur hier beschriebenen winkelstabilen Technik wurde früher meist mittels Winkelplatte korrigiert.
Weiterbehandlung: Mobilisation unter Abrollbelastung an 2 Gehstöcken über 6 Wochen. Röntgenkontrolle und bei genügender Knochenkonsolidation Steigerung der Belastung. Implantatentfernung nach 9 bis 12 Monaten. Rückkehr zum Sport ab 3 Monaten.
Ergebnisse: Die PVO ist eine in der Behandlung von LCPD nahezu seit 60 Jahren angewendete und weltweit etablierte chirurgische Technik. Durch ein stetig wachsendes Verständnis der Grunderkrankung wird einerseits die Indikationsstellung für operative Interventionen optimiert. Andererseits tragen neue Implantate zur Verbesserung der klinisch-radiologischen Resultate und Verringerung von Komplikationen während und nach Operation bei.
Keywords: Correction angle; Femoral osteotomy; LCP pediatric hip plate; LCPD; Pediatric hip; Perthes.
© 2022. The Author(s).










Similar articles
-
[Triple osteotomy for patients with Legg-Calve-Perthes disease].Oper Orthop Traumatol. 2022 Oct;34(5):323-332. doi: 10.1007/s00064-022-00784-5. Epub 2022 Sep 16. Oper Orthop Traumatol. 2022. PMID: 36112163 Free PMC article. Review. German.
-
Lateral acetabular growth stimulation following a labral support procedure in Legg-Calve-Perthes disease.J Bone Joint Surg Am. 2006 Jul;88(7):1458-66. doi: 10.2106/JBJS.E.00689. J Bone Joint Surg Am. 2006. PMID: 16818970
-
Outcomes of Combined Shelf Acetabuloplasty with Femoral Varus Osteotomy in Severe Legg-Calve-Perthes (LCP) Disease: Advanced Containment Method for Severe LCP Disease.Clin Orthop Surg. 2015 Dec;7(4):497-504. doi: 10.4055/cios.2015.7.4.497. Epub 2015 Nov 13. Clin Orthop Surg. 2015. PMID: 26640634 Free PMC article.
-
Head reduction osteotomy with additional containment surgery improves sphericity and containment and reduces pain in Legg-Calvé-Perthes disease.Clin Orthop Relat Res. 2015 Apr;473(4):1274-83. doi: 10.1007/s11999-014-4048-1. Clin Orthop Relat Res. 2015. PMID: 25384430 Free PMC article.
-
Salter osteotomy in Legg-Calvé-Perthes disease.J Pediatr Orthop. 2011 Sep;31(2 Suppl):S192-7. doi: 10.1097/BPO.0b013e318223b59d. J Pediatr Orthop. 2011. PMID: 21857438 Review.
Cited by
-
Modified Trochanteric Flip Osteotomy in Varus Intertrochanteric Osteotomy for Treatment of Legg-Calvé-Perthes Disease.Children (Basel). 2025 Jan 1;12(1):51. doi: 10.3390/children12010051. Children (Basel). 2025. PMID: 39857882 Free PMC article.
References
-
- Rab GT. Biomechanical aspects of Salter osteotomy. Clin Orthop Relat Res. 1978;132:82–87. - PubMed
-
- Sankar WN, Lavalva SM, Mcguire MF, Jo C, Laine JC, Kim HKW, International Perthes Study Group Does early proximal femoral varus osteotomy shorten the duration of fragmentation in Perthes disease? Lessons from a prospective multicenter cohort. J Pediatr Orthop. 2020;40(5):e322–e328. doi: 10.1097/BPO.0000000000001451. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
