

Modeling the impact of COVID-19 pandemic-driven increases in alcohol consumption on health outcomes and hospitalization costs in the United States
- PMID: 35915549
- PMCID: PMC9539393
- DOI: 10.1111/add.16018
Modeling the impact of COVID-19 pandemic-driven increases in alcohol consumption on health outcomes and hospitalization costs in the United States
Abstract
Background and aims: Alcohol consumption increased in the early phases of the COVID-19 pandemic in the United States. Alcohol use disorder (AUD) and risky drinking are linked to harmful health effects. This paper aimed to project future health and cost impacts of shifts in alcohol consumption during the COVID-19 pandemic.
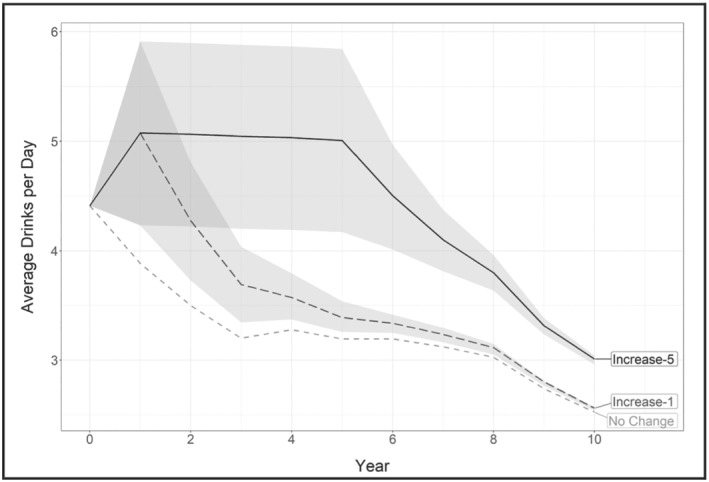
Design: An individual-level simulation model of the long-term drinking patterns for people with life-time AUD was used to simulate 10 000 individuals and project model outcomes to the estimated 25.9 million current drinkers with life-time AUD in the United States. The model considered three scenarios: (1) no change (counterfactual for comparison); (2) increased drinking levels persist for 1 year ('increase-1') and (3) increased drinking levels persist for 5 years ('increase-5').
Setting: United States.
Participants: Current drinkers with life-time AUD.
Measurements: Life expectancy [life-years (LYs)], quality-adjusted life-years (QALYs), alcohol-related hospitalizations and associated hospitalization costs and alcohol-related deaths, during a 5-year period.
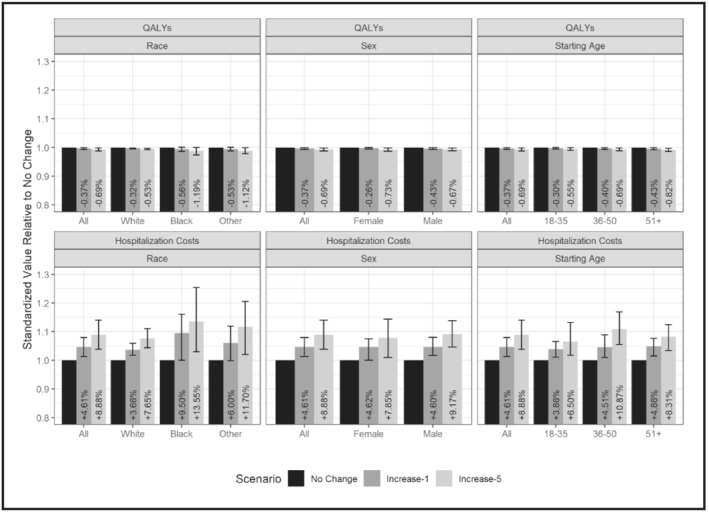
Findings: Short-term increases in alcohol consumption (increase-1 scenario) resulted in a loss of 79 000 [95% uncertainty interval (UI]) 26 000-201 000] LYs, a loss of 332 000 (104 000-604 000) QALYs and 295 000 (82 000-501 000) more alcohol-related hospitalizations, costing an additional $5.4 billion ($1.5-9.3 billion) over 5 years. Hospitalizations for cirrhosis of the liver accounted for approximately $3.0 billion ($0.9-4.8 billion) in hospitalization costs, more than half the increase across all alcohol-related conditions. Health and cost impacts were more pronounced for older age groups (51+), women and non-Hispanic black individuals. Increasing the duration of pandemic-driven increases in alcohol consumption in the increase-5 scenario resulted in larger impacts.
Conclusions: Simulations show that if the increase in alcohol consumption observed in the United States in the first year of the pandemic continues, alcohol-related mortality, morbidity and associated costs will increase substantially over the next 5 years.
Keywords: COVID-19; alcohol consumption; alcohol use disorder; alcohol-related hospitalizations; alcohol-related liver disease; alcohol-related morbidity and mortality; health utility; hospitalization cost; simulation model.
© 2022 Society for the Study of Addiction.
Figures
References
-
- North CS, Ringwalt CL, Downs D, Derzon J, Galvin D. Postdisaster course of alcohol use disorders in systematically studied survivors of 10 disasters. Arch Gen Psychiatry. 2011;68:173–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
