

Effectiveness of Multimodal Chiropractic Care Featuring Spinal Manipulation for Persistent Spinal Pain Syndrome Following Lumbar Spine Surgery: Retrospective Chart Review of 31 Adults in Hong Kong
- PMID: 35915570
- PMCID: PMC9357349
- DOI: 10.12659/MSM.937640
Effectiveness of Multimodal Chiropractic Care Featuring Spinal Manipulation for Persistent Spinal Pain Syndrome Following Lumbar Spine Surgery: Retrospective Chart Review of 31 Adults in Hong Kong
Abstract
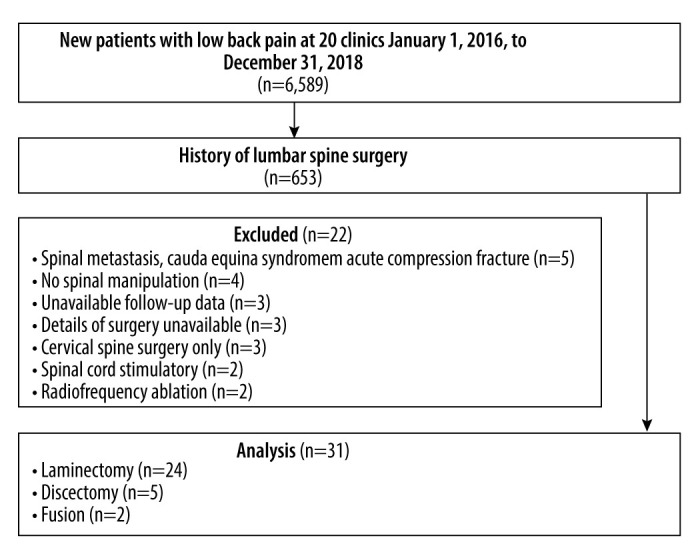
BACKGROUND The term "persistent spinal pain syndrome type 2" (PSPS-2) has been proposed by the International Association for the Study of Pain to replace the term "failed back surgery syndrome". This retrospective study aimed to evaluate effectiveness of multimodal care featuring chiropractic spinal manipulation (CSMT) in 31 adults in Hong Kong with PSPS-2. MATERIAL AND METHODS We identified new adult patients with PSPS-2 receiving CSMT from 2016 to 2018. Demographic and clinical data and baseline/follow-up numeric pain rating scale (NPRS) and Oswestry Disability Index (ODI) scores were extracted. Multiple linear regression was used to examine posttreatment NPRS and ODI reduction, with clinical variables as covariates. RESULTS Of 6589 patients with low back pain, 31 met criteria (mean age 52.2±13.7 years). Surgeries included laminectomy (81%), discectomy (13%), and fusion (6%). Mean baseline NRPS was 6.6±1.9; ODI was 43.8±15.1%. Patients received CSMT (100%), drop technique (81%), passive modalities (65%), soft tissue manipulation (13%), flexion-distraction (13%), and mechanical traction (13%). Mean posttreatment NPRS was 0.6±1.0; ODI was 2.4±3.3%. All patients had a minimum clinically important difference for NPRS (≥2/10) and ODI (≥30%). One year after treatment, 48% maintained improvement, 42% experienced recurrence; in 10%, follow-up was unavailable. Regression analysis identified younger age, shorter symptom duration, and greater baseline NPRS as predictors of NPRS reduction; and greater baseline ODI as a predictor of ODI reduction (all P<0.05). CONCLUSIONS Patients with PSPS-2 improved with multimodal care featuring CSMT, which was more effective in patients with younger age, shorter symptom duration, and higher baseline pain or disability levels.
Conflict of interest statement
Figures




Similar articles
-
Chiropractic management of postsurgical lumbar spine pain: a retrospective study of 32 cases.J Manipulative Physiol Ther. 2011 Jul-Aug;34(6):408-12. doi: 10.1016/j.jmpt.2011.05.011. J Manipulative Physiol Ther. 2011. PMID: 21807265
-
The association between individual radiographic findings and improvement after chiropractic spinal manipulation and home exercise among older adults with back-related disability: a secondary analysis.Chiropr Man Therap. 2025 Jan 7;33(1):2. doi: 10.1186/s12998-024-00566-9. Chiropr Man Therap. 2025. PMID: 39773270 Free PMC article. Clinical Trial.
-
Short-term effectiveness of spinal manipulative therapy versus functional technique in patients with chronic nonspecific low back pain: a pragmatic randomized controlled trial.Spine J. 2016 Mar;16(3):302-12. doi: 10.1016/j.spinee.2015.08.057. Epub 2015 Sep 8. Spine J. 2016. PMID: 26362233 Clinical Trial.
-
Metastatic Recurrent Breast Cancer Identified in the Chiropractic Office: Case Report and Literature Review.Am J Case Rep. 2022 Sep 4;23:e937609. doi: 10.12659/AJCR.937609. Am J Case Rep. 2022. PMID: 36057783 Free PMC article. Review.
-
Clinical Patient-Relevant Outcome Domains for Persistent Spinal Pain Syndrome-A Scoping Review and Expert Panels.J Clin Med. 2024 Mar 28;13(7):1975. doi: 10.3390/jcm13071975. J Clin Med. 2024. PMID: 38610739 Free PMC article.
Cited by
-
Patients With a History of Spine Surgery Receiving Chiropractic Spinal Manipulation in US Academic Health Centers: A Cross-Sectional Cohort Study.Cureus. 2023 Apr 6;15(4):e37216. doi: 10.7759/cureus.37216. eCollection 2023 Apr. Cureus. 2023. PMID: 37159789 Free PMC article.
-
Colorectal Cancer Presenting as Sacral Pain at a Chiropractic Clinic.Cureus. 2023 May 20;15(5):e39277. doi: 10.7759/cureus.39277. eCollection 2023 May. Cureus. 2023. PMID: 37346203 Free PMC article.
-
Multimodal management for low-back pain associated with spondylodiscitis.Med Pharm Rep. 2024 Oct;97(4):557-561. doi: 10.15386/mpr-2582. Epub 2024 Oct 30. Med Pharm Rep. 2024. PMID: 39502759 Free PMC article.
-
Association between spinal manipulative therapy and lumbar spine reoperation after discectomy: a retrospective cohort study.BMC Musculoskelet Disord. 2024 Jan 10;25(1):46. doi: 10.1186/s12891-024-07166-x. BMC Musculoskelet Disord. 2024. PMID: 38200469 Free PMC article.
-
Improvement of Chronic Neck Pain After Posterior Atlantoaxial Surgical Fusion via Multimodal Chiropractic Care: A Case Report.Cureus. 2023 Feb 4;15(2):e34630. doi: 10.7759/cureus.34630. eCollection 2023 Feb. Cureus. 2023. PMID: 36891015 Free PMC article.
References
-
- Al Kaisy A, Pang D, Desai MJ, et al. Failed back surgery syndrome: Who has failed? Neurochirurgie. 2015;61(Suppl 1):S6–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
