

Brain and Adrenal Metastasis From Unknown Primary Tumor: A Case Report
- PMID: 35915686
- PMCID: PMC9337777
- DOI: 10.7759/cureus.26438
Brain and Adrenal Metastasis From Unknown Primary Tumor: A Case Report
Abstract
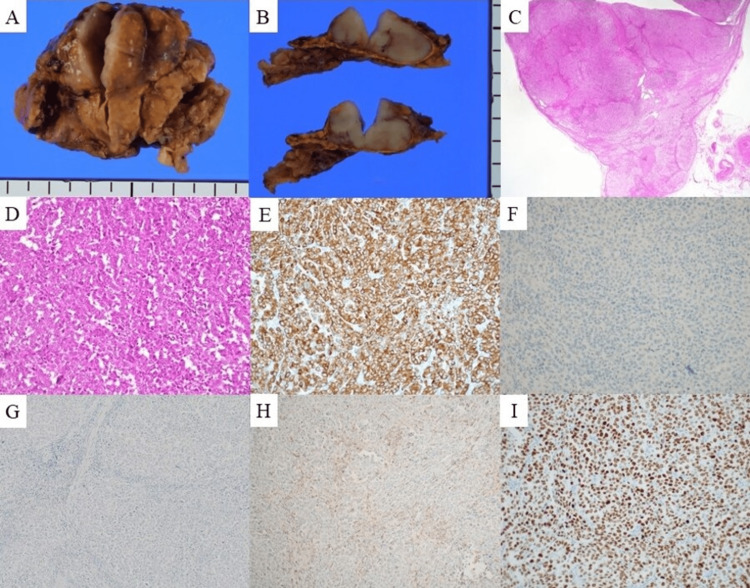
The clinical management of brain metastasis (BM) and adrenal metastasis (AM) of cancer of unknown primary (CUP) can be challenging. A 73-year-old man presented to the hospital with sudden-onset hemiplegia. His laboratory data were normal, except for elevated levels of carcinoembryonic antigen (CEA) (33.8 ng/mL). Contrast-enhanced magnetic resonance imaging revealed a 2-cm mass with ring enhancement in the right parietal lobe and extensive vasogenic edema around the tumor. The lesion was diagnosed as BM; however, we could not detect the primary origin by fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET-CT). Stereotactic radiotherapy was then administered, resulting in reduced tumor size and relief of symptoms. Follow-up after one year revealed an elevated CEA level (148.6 ng/mL) and remarkable fluorodeoxyglucose (FDG) uptake in the right adrenal gland, with an area of enhancement of 20 mm, on FDG-positron emission tomography computed tomography, with normal findings in other distant organs. He underwent adrenalectomy, and the adrenal tumor was diagnosed as a poorly differentiated adenocarcinoma likely of lung origin based on the histopathologic and immunohistochemistry findings of cytokeratin (CK) 7 (+), CK 20 (-), thyroid transcription factor-1 (TTF-1) (+), inhibin (-), napsin A (+), prostate-specific antigen (PSA) (-), caudal type homeobox 2 (CDX-2) (-), synaptophysin (-), and p40 (-). Metastatic tumors of unknown primary origin remain latent. Aggressive treatment of these lesions can be beneficial for symptom relief, diagnosis, and prolongation of survival.
Keywords: adrenal metastasis of unknown primary; brain metastasis of unknown primary; cancer of unknown primary; carcinoembryonic antigen; stereotactic radiotherapy.
Copyright © 2022, Katsumata et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Initial clinical presentation of single soft tissue metastasis of medullary thyroid carcinoma without primary tumor in the thyroid gland.World J Surg Oncol. 2017 Dec 13;15(1):221. doi: 10.1186/s12957-017-1293-2. World J Surg Oncol. 2017. PMID: 29237502 Free PMC article.
-
A case of primary lung cancer lesion demonstrated by F-18 FDG positron emission tomography/computed tomography (PET/CT) one year after the detection of metastatic brain tumor.Oncol Lett. 2011 Jul;2(4):621-623. doi: 10.3892/ol.2011.318. Epub 2011 May 16. Oncol Lett. 2011. PMID: 22848237 Free PMC article.
-
[A case of long-term survival after resection for postoperative solitary adrenal metastasis from esophageal adenocarcinoma].Gan To Kagaku Ryoho. 2010 Nov;37(12):2406-8. Gan To Kagaku Ryoho. 2010. PMID: 21224588 Review. Japanese.
-
Imaging and management of a small cell lung cancer metastasis/adrenal adenoma collision tumor: a case report and review of the literature.World J Surg Oncol. 2014 Feb 26;12:45. doi: 10.1186/1477-7819-12-45. World J Surg Oncol. 2014. PMID: 24571800 Free PMC article. Review.
Cited by
-
A Unique Case of Poorly Differentiated Neuroendocrine Carcinoma With Brain and Bilateral Adrenal Metastases.Cancer Rep (Hoboken). 2025 Feb;8(2):e70130. doi: 10.1002/cnr2.70130. Cancer Rep (Hoboken). 2025. PMID: 39894895 Free PMC article.
References
-
- Brain metastases. Achrol AS, Rennert RC, Anders C, et al. Nat Rev Dis Primers. 2019;5 - PubMed
-
- Brain metastases as the only manifestation of an undetected primary tumor. Nguyen LN, Maor MH, Oswald MJ. Cancer. 1998;83:2181–2184. - PubMed
-
- Unknown primary cancer presenting as an adrenal mass: frequency and implications for diagnostic evaluation of adrenal incidentalomas. Lee JE, Evans DB, Hickey RC, Sherman SI, Gagel RF, Abbruzzese MC, Abbruzzese JL. Surgery. 1998;124:1115–1122. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous