

A Gene Expression Signature to Select Hepatocellular Carcinoma Patients for Liver Transplantation
- PMID: 35916378
- PMCID: PMC9534058
- DOI: 10.1097/SLA.0000000000005637
A Gene Expression Signature to Select Hepatocellular Carcinoma Patients for Liver Transplantation
Abstract
Objective: To propose a new decision algorithm combining biomarkers measured in a tumor biopsy with clinical variables, to predict recurrence after liver transplantation (LT).
Background: Liver cancer is one of the most frequent causes of cancer-related mortality. LT is the best treatment for hepatocellular carcinoma (HCC) patients but the scarcity of organs makes patient selection a critical step. In addition, clinical criteria widely applied in patient eligibility decisions miss potentially curable patients while selecting patients that relapse after transplantation.
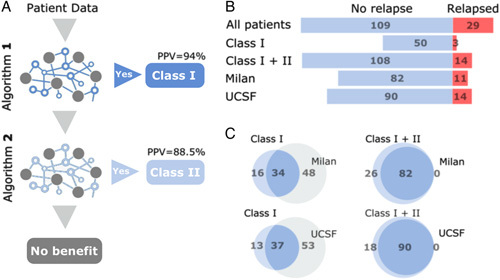
Methods: A literature systematic review singled out candidate biomarkers whose RNA levels were assessed by quantitative PCR in tumor tissue from 138 HCC patients submitted to LT (>5 years follow up, 32% beyond Milan criteria). The resulting 4 gene signature was combined with clinical variables to develop a decision algorithm using machine learning approaches. The method was named HepatoPredict.
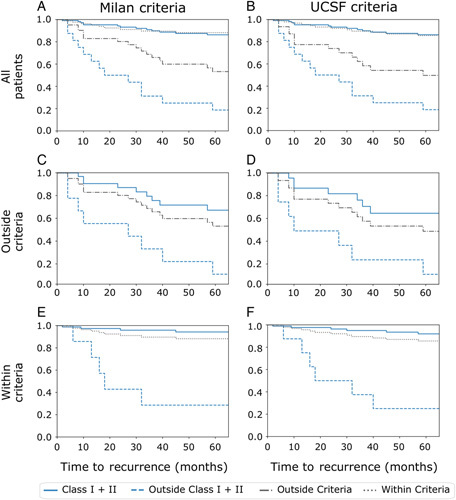
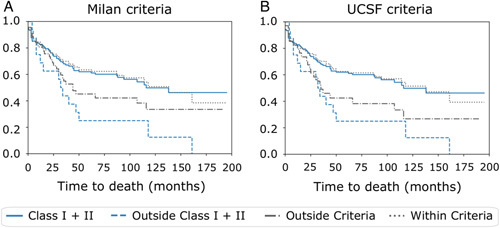
Results: HepatoPredict identifies 99% disease-free patients (>5 year) from a retrospective cohort, including many outside clinical criteria (16%-24%), thus reducing the false negative rate. This increased sensitivity is accompanied by an increased positive predictive value (88.5%-94.4%) without any loss of long-term overall survival or recurrence rates for patients deemed eligible by HepatoPredict; those deemed ineligible display marked reduction of survival and increased recurrence in the short and long term.
Conclusions: HepatoPredict outperforms conventional clinical-pathologic selection criteria (Milan, UCSF), providing superior prognostic information. Accurately identifying which patients most likely benefit from LT enables an objective stratification of waiting lists and information-based allocation of optimal versus suboptimal organs.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, et al. . Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Saito R, Amemiya H, Hosomura N, et al. . Prognostic factors for post-recurrent survival in hepatocellular carcinoma after curative resection. Anticancer Res. 2019;39:3033–3038. - PubMed
-
- Mazzaferro V, Regalia E, Doci R, et al. . Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–700. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
