

Time is tissue: Barriers to timely transfusion after pediatric injury
- PMID: 35916621
- PMCID: PMC9805480
- DOI: 10.1097/TA.0000000000003752
Time is tissue: Barriers to timely transfusion after pediatric injury
Abstract
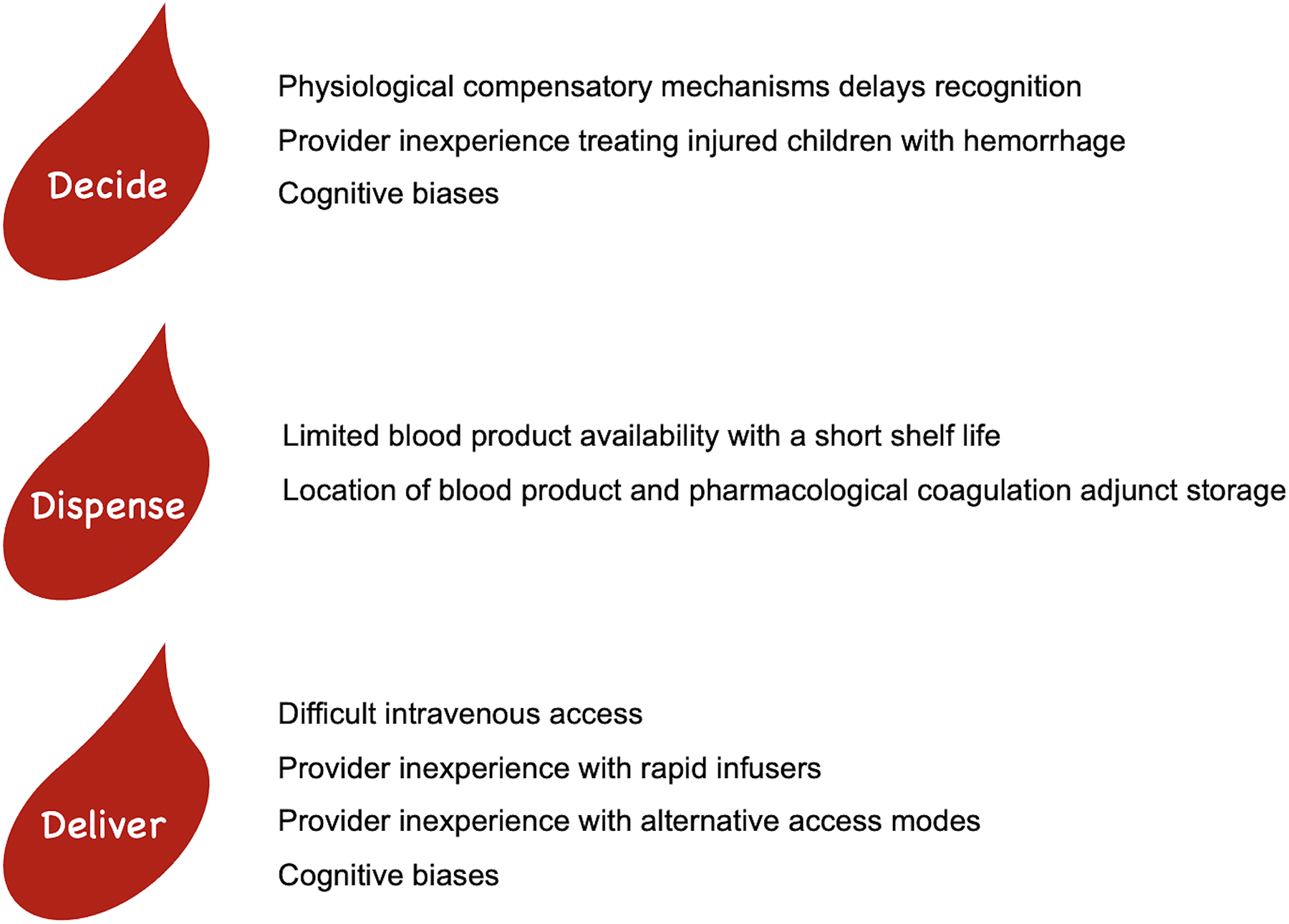
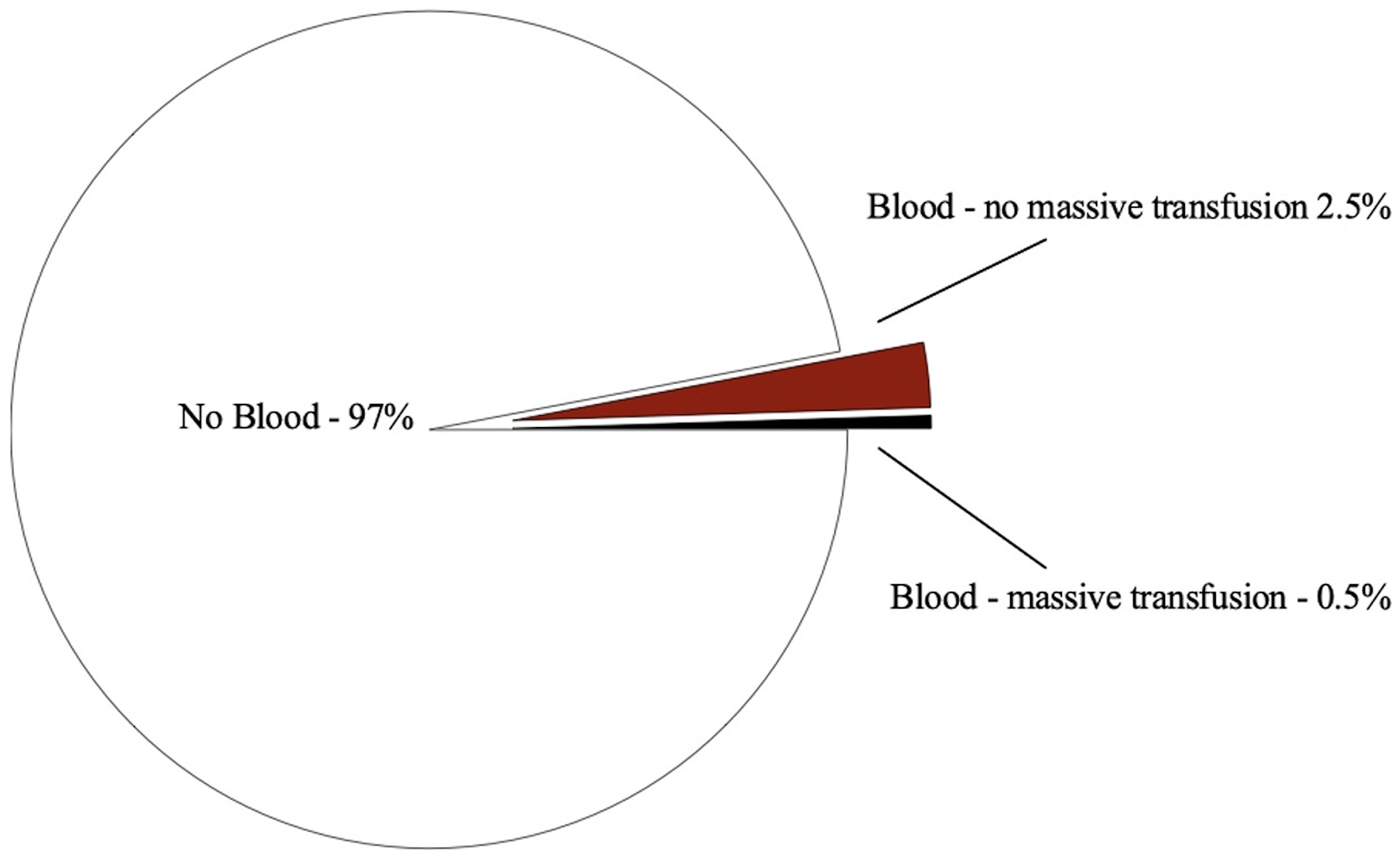
Strategies to improve outcomes among children and adolescents in hemorrhagic shock have primarily focused on component resuscitation, pharmaceutical coagulation adjuncts, and hemorrhage control techniques. Many of these strategies have been associated with better outcomes in children, but the barriers to their use and the impact of timely use on morbidity and mortality have received little attention. Because transfusion is uncommon in injured children, few studies have identified and described barriers to the processes of using these interventions in bleeding patients, processes that move from the decision to transfuse, to obtaining the necessary blood products and adjuncts, and to delivering them to the patient. In this review, we identify and describe the steps needed to ensure timely blood transfusion and propose practices to minimize barriers in this process. Given the potential impact of time on hemorrhage associated outcomes, ensuring timely intervention may have a similar or greater impact than the interventions themselves.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
Figures

References
-
- Acosta JA, Yang JC, Winchell RJ, Simons RK, Fortlage DA, Hollingsworth-Fridlund P, et al. Lethal injuries and time to death in a level I trauma center. J Am Coll Surg. 1998;186(5):528–33. - PubMed
-
- Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. J Trauma. 2006;60(6 Suppl):S3–11. - PubMed
-
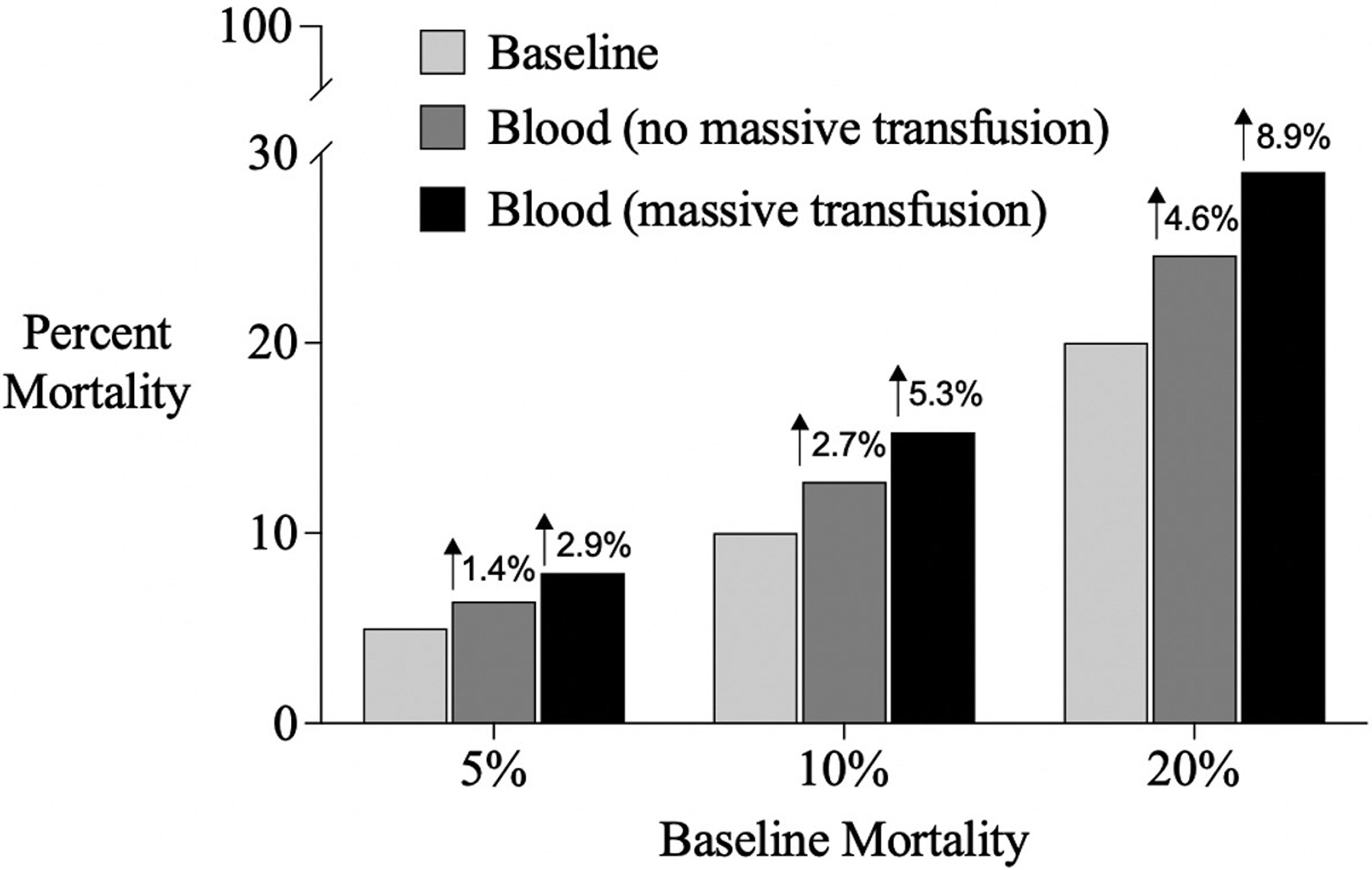
- Reppucci ML, Pickett K, Stevens J, Phillips R, Recicar J, Annen K, et al. Massive transfusion in pediatric trauma-does more blood predict mortality? J Pediatr Surg. 2022;57(2):308–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
