

Maternal pre-pregnancy/early-pregnancy smoking and risk of congenital heart diseases in offspring: A prospective cohort study in Central China
- PMID: 35916623
- PMCID: PMC9344981
- DOI: 10.7189/jogh.12.11009
Maternal pre-pregnancy/early-pregnancy smoking and risk of congenital heart diseases in offspring: A prospective cohort study in Central China
Abstract
Background: Prior studies suggested that maternal smoking before and during pregnancy could be associated with increased risks of congenital heart diseases (CHDs) in offspring. However, the results were inconsistent, and the existence of a causal relationship was not confirmed. Our study aimed to estimate the associations of maternal active and passive smoking during the pre-pregnancy/early-pregnancy period with CHDs as well as its common phenotypes in offspring.
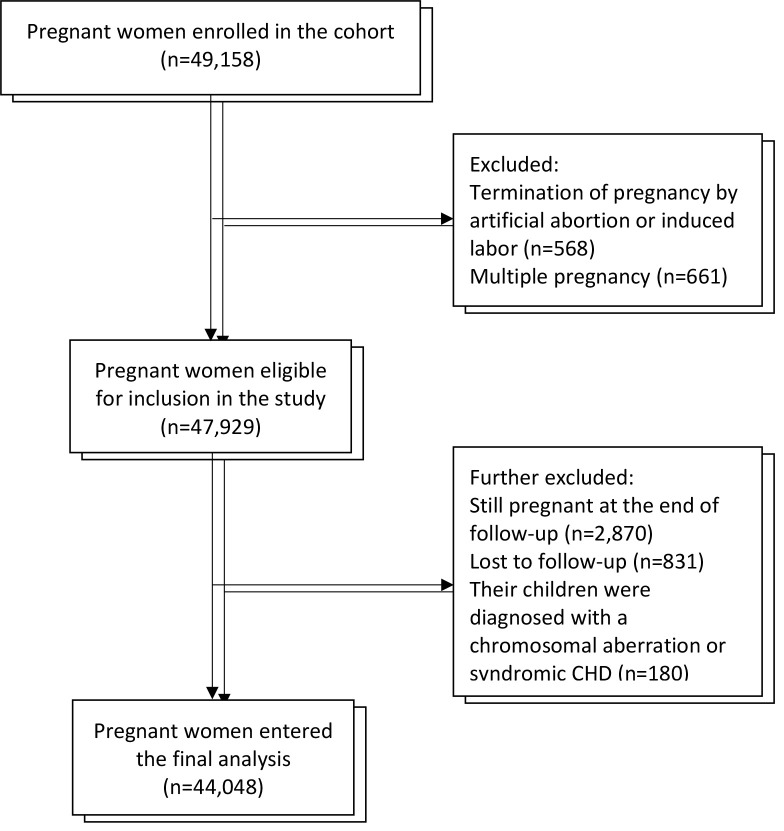
Methods: This study was based on data from a prospective cohort study conducted in Central China. A total of 49 158 eligible pregnant women between the 8th and 14th weeks of gestation were invited to join the cohort and were planned to be followed up until 3 months postpartum. The exposure of interest was maternal smoking status, including active and passive smoking status in 3 months before pregnancy as well as in early pregnancy. Self-reported maternal smoking status was ascertained via an in-person interview after recruitment. CHDs were diagnosed by pediatric cardiologists and classified according to ICD-10. Multivariable Poisson regression models were used to estimate the relative risks (RRs) with 95% confidence intervals (CIs) of all CHDs and their common phenotypes associated with maternal smoking status, adjusting for potential confounding factors identified by directed acyclic graphs.
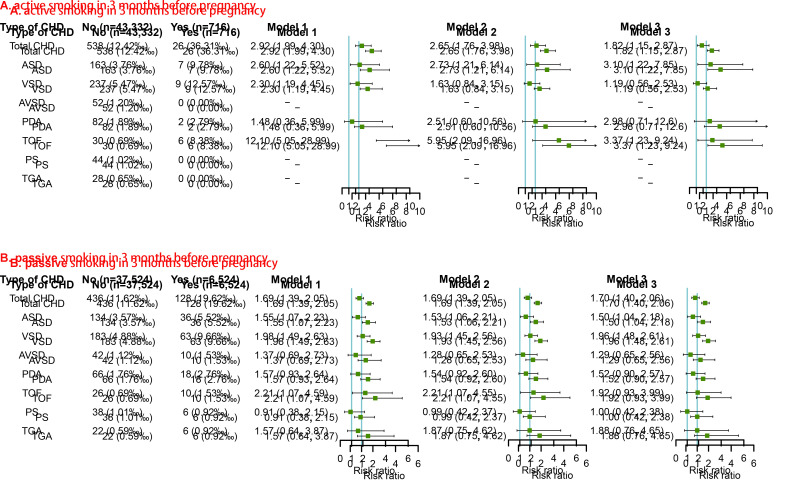
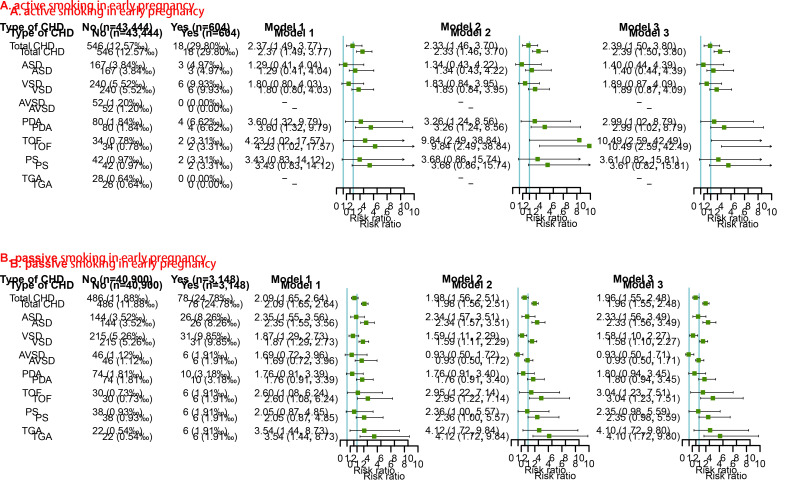
Results: CHDs were diagnosed in 564 children. After adjusting for potential confounding factors and comparing with the unexposed groups, CHDs incidence was 165% higher (adjusted RR = 2.65; 95% CI = 1.76-3.98) in offspring exposed to maternal active smoking in 3 months before pregnancy, 69% higher (adjusted-RR = 1.69; 95% CI = 1.39-2.05) in offspring exposed to maternal passive smoking in 3 months before pregnancy, 133% higher (adjusted RR = 2.33; 95% CI = 1.46-3.70) for offspring exposed to maternal active smoking in early pregnancy, and 98% higher (adjusted-RR = 1.98; 95% CI = 1.56-2.51) for offspring exposed to maternal passive smoking in early pregnancy. More specifically, the offspring exposed to maternal active smoking in early pregnancy had the highest risk of Tetralogy of Fallot (adjusted RR = 9.84; 95% CI = 2.49-38.84). These findings were recapitulated in analyses that further adjusted for other behaviour variables apart from the characteristic being assessed and were also confirmed by sensitivity analyses.
Conclusions: Our findings add to the existing body of evidence that implicates maternal pre-pregnancy/early-pregnancy smoking as a significant risk factor for CHDs and their select phenotypes.
Copyright © 2022 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding authors) and declare no relevant interest.
Figures
Similar articles
-
Effect of maternal alcohol consumption during the pre-pregnancy/early-pregnancy period on congenital heart disease: A prospective cohort study in Central China.Prev Med. 2022 Feb;155:106963. doi: 10.1016/j.ypmed.2022.106963. Epub 2022 Jan 20. Prev Med. 2022. PMID: 35065976
-
Parental smoking and the risk of congenital heart defects in offspring: An updated meta-analysis of observational studies.Eur J Prev Cardiol. 2020 Aug;27(12):1284-1293. doi: 10.1177/2047487319831367. Epub 2019 Mar 23. Eur J Prev Cardiol. 2020. PMID: 30905164 Review.
-
Maternal Viral Infection in Early Pregnancy and Risk of Congenital Heart Disease in Offspring: A Prospective Cohort Study in Central China.Clin Epidemiol. 2022 Jan 18;14:71-82. doi: 10.2147/CLEP.S338870. eCollection 2022. Clin Epidemiol. 2022. PMID: 35082532 Free PMC article.
-
[Association between maternal passive smoking during perinatal period and congenital heart disease in their offspring-based on a case-control study].Zhonghua Liu Xing Bing Xue Za Zhi. 2020 Jun 10;41(6):884-889. doi: 10.3760/cma.j.cn112338-20190710-00509. Zhonghua Liu Xing Bing Xue Za Zhi. 2020. PMID: 32564554 Chinese.
-
Risks of specific congenital anomalies in offspring of women with diabetes: A systematic review and meta-analysis of population-based studies including over 80 million births.PLoS Med. 2022 Feb 1;19(2):e1003900. doi: 10.1371/journal.pmed.1003900. eCollection 2022 Feb. PLoS Med. 2022. PMID: 35104296 Free PMC article.
Cited by
-
The Impact of Prenatal Environmental Tobacco Smoking (ETS) and Exposure on Chinese Children: A Systematic Review.Children (Basel). 2023 Aug 7;10(8):1354. doi: 10.3390/children10081354. Children (Basel). 2023. PMID: 37628353 Free PMC article. Review.
-
The impact of maternal health and lifestyle on low birth weight: a prospective cohort study.Ital J Pediatr. 2025 Jul 10;51(1):217. doi: 10.1186/s13052-025-02080-x. Ital J Pediatr. 2025. PMID: 40640972 Free PMC article.
-
Comparison of secular trends of leukemia in China and the United States from 1990 to 2021 and their projections for the next 15 years.Front Public Health. 2024 Aug 16;12:1425043. doi: 10.3389/fpubh.2024.1425043. eCollection 2024. Front Public Health. 2024. PMID: 39220457 Free PMC article.
-
The impact of in utero tobacco exposure on smoking behaviors, cardiovascular disease risk and all-cause mortality in adulthood: A UK Biobank study.Curr Res Toxicol. 2025 Feb 23;8:100226. doi: 10.1016/j.crtox.2025.100226. eCollection 2025. Curr Res Toxicol. 2025. PMID: 40109875 Free PMC article.
-
Association of secondhand smoke exposure during pregnancy with left ventricle structure and function in offspring at 4 years old: a prospective birth cohort study.BMC Pregnancy Childbirth. 2025 Apr 29;25(1):515. doi: 10.1186/s12884-025-07636-7. BMC Pregnancy Childbirth. 2025. PMID: 40301798 Free PMC article.
References
-
- World Health Organization. Women and the Tobacco Epidemic: Challenges for the 21st Century. Geneva: World Health Organization; 2001.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
