

Glomerular filtration rate in critically ill neonates and children: creatinine-based estimations versus iohexol-based measurements
- PMID: 35916956
- PMCID: PMC9925555
- DOI: 10.1007/s00467-022-05651-w
Glomerular filtration rate in critically ill neonates and children: creatinine-based estimations versus iohexol-based measurements
Abstract
Background: Acute kidney injury (AKI) and augmented renal clearance (ARC), both alterations of the glomerular filtration rate (GFR), are prevalent in critically ill children and neonates. AKI and ARC prevalence estimates are based on estimation of GFR (eGFR) using serum creatinine (SCr), which is known to be inaccurate. We aimed to test our hypothesis that AKI prevalence will be higher and ARC prevalence will be lower in critically ill children when using iohexol-based measured GFR (mGFR), rather than using eGFR. Additionally, we aimed to investigate the performance of different SCr-based eGFR methods.
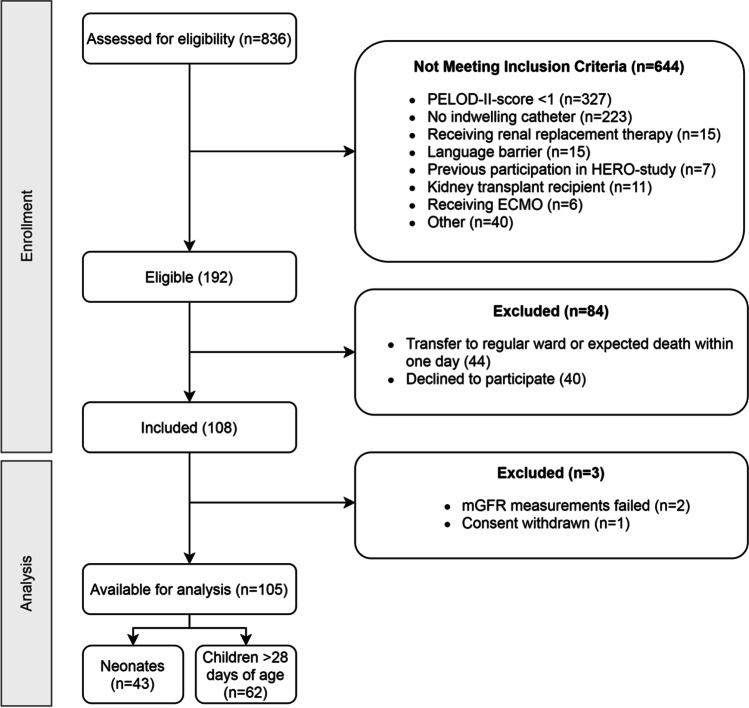
Methods: In this single-center prospective study, critically ill term-born neonates and children were included. mGFR was calculated using a plasma disappearance curve after parenteral administration of iohexol. AKI diagnosis was based on the KDIGO criteria, SCr-based eGFR, and creatinine clearance (CrCL). Differences between eGFR and mGFR were determined using Wilcoxon signed-rank tests and by calculating bias and accuracy (percentage of eGFR values within 30% of mGFR values).
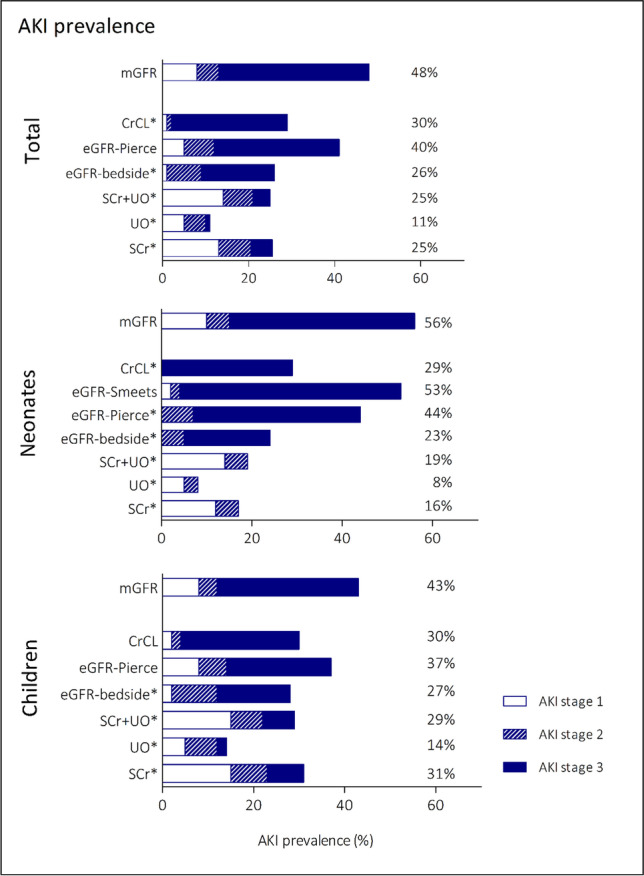
Results: One hundred five children, including 43 neonates, were included. AKI prevalence was higher based on mGFR (48%), than with KDIGO or eGFR (11-40%). ARC prevalence was lower with mGFR (24%) compared to eGFR (38-51%). eGFR equations significantly overestimated mGFR (60-71 versus 41 ml/min/1.73 m2, p < 0.001-0.002). Accuracy was highest with eGFR equations based on age- and sex-dependent equations (up to 59%).
Conclusion: Iohexol-based AKI prevalence was higher and ARC prevalence lower compared to standard SCr-based eGFR methods. Age- and sex-dependent equations for eGFR (eGFR-Smeets for neonates and eGFR-Pierce for children) best approached measured GFR and should preferably be used to optimize diagnosis of AKI and ARC in this population. A higher resolution version of the Graphical abstract is available as Supplementary information.
Keywords: Acute kidney injury; Augmented renal clearance; Creatinine; Creatinine clearance; Glomerular filtration rate; Iohexol.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
