

Magnetic resonance imaging findings of cystic ovarian tumors: major differential diagnoses in five types frequently encountered in daily clinical practice
- PMID: 35916971
- PMCID: PMC9719891
- DOI: 10.1007/s11604-022-01321-x
Magnetic resonance imaging findings of cystic ovarian tumors: major differential diagnoses in five types frequently encountered in daily clinical practice
Abstract
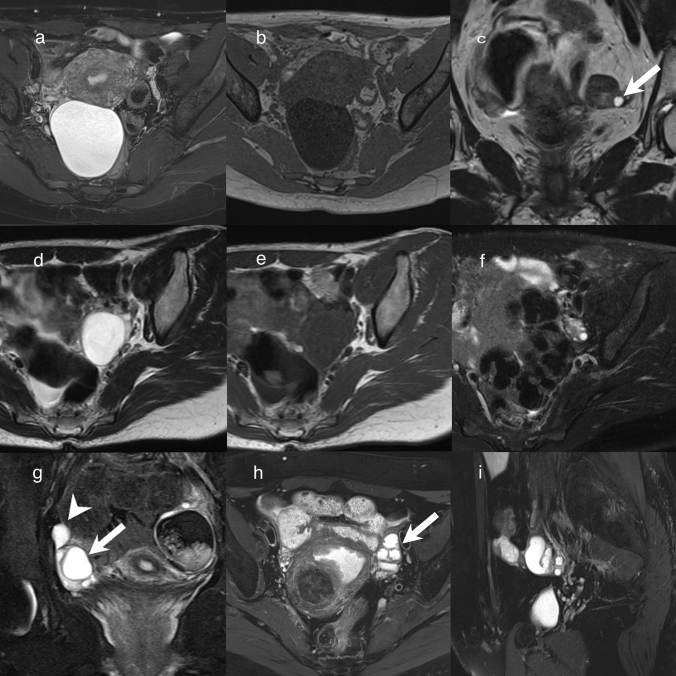
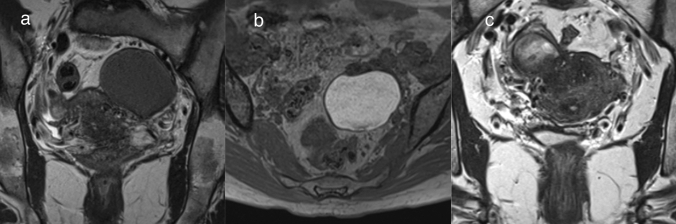
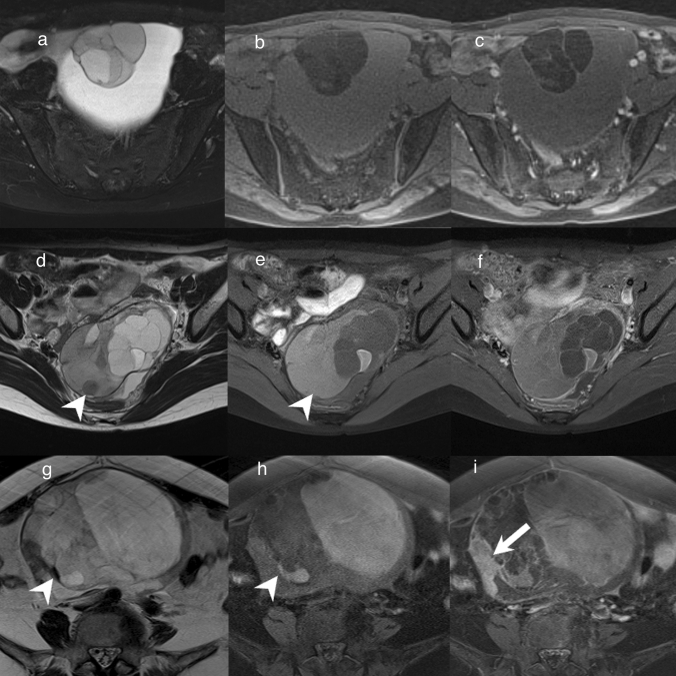
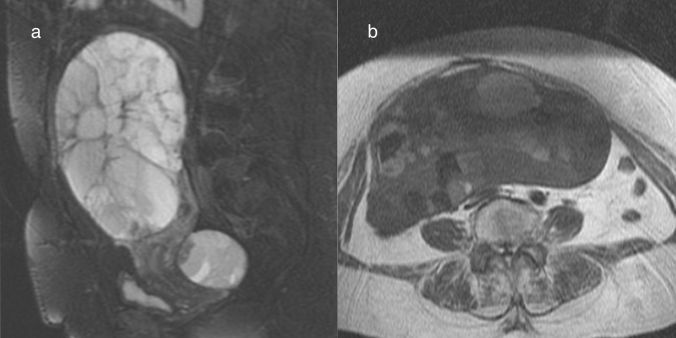
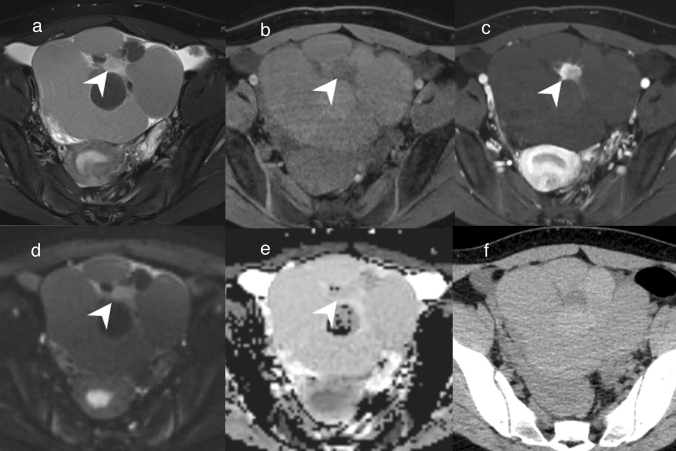
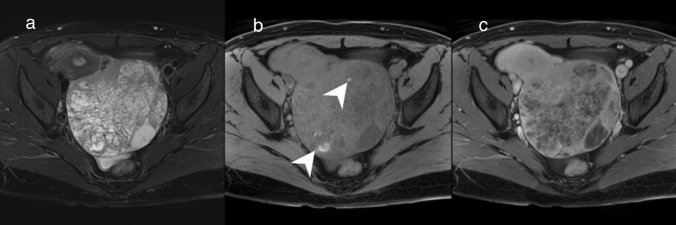
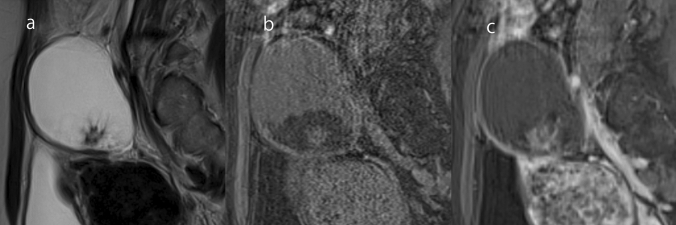
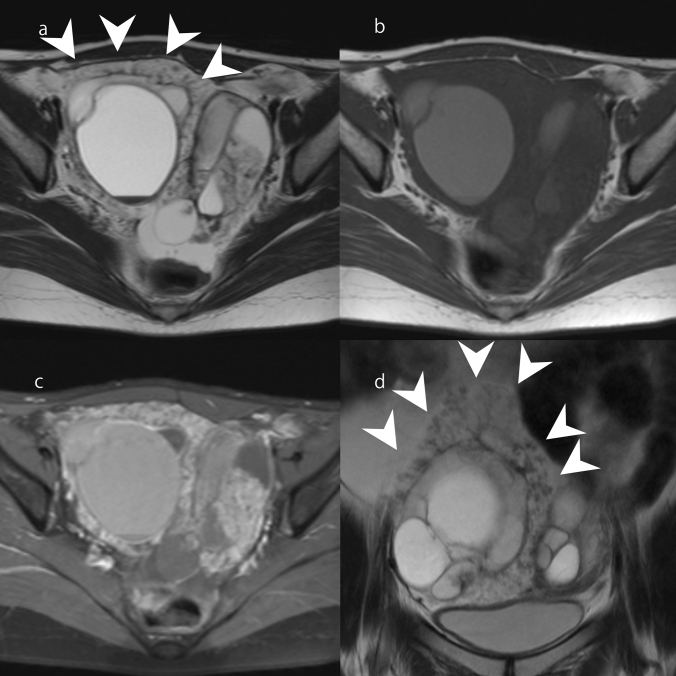
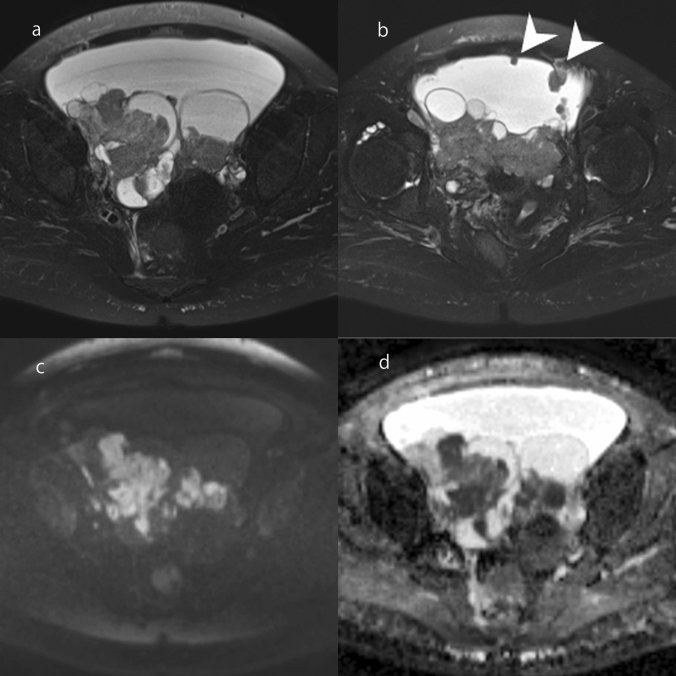
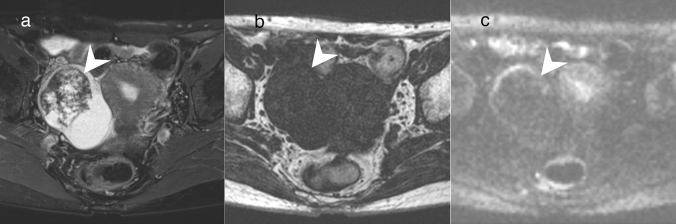
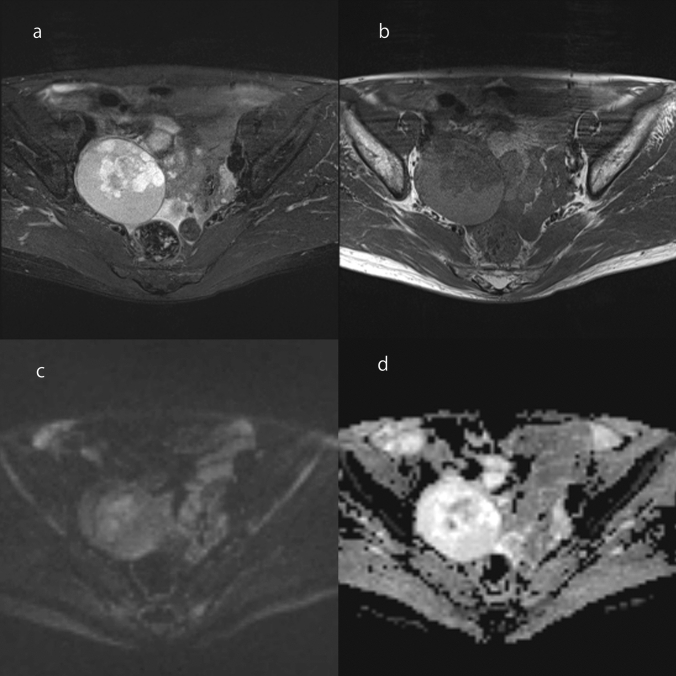
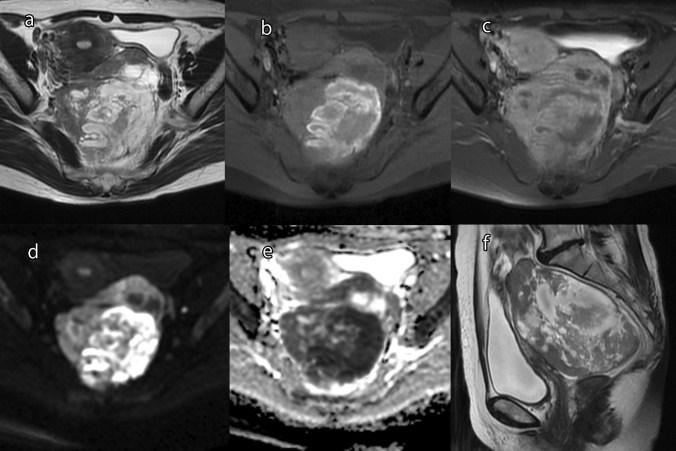
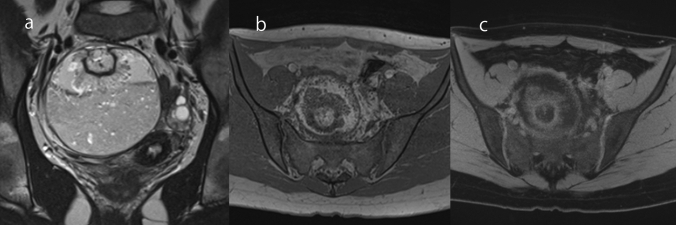
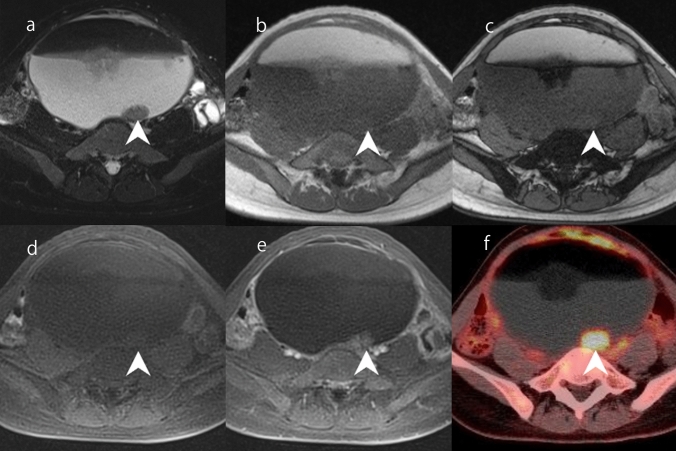
There are many types of ovarian tumors, and these different types often form cystic masses with a similar appearance, which can make their differentiation difficult. However, with the exclusion of rare ovarian tumors, the number of ovarian tumors encountered in daily practice is somewhat fixed. It goes without saying that magnetic resonance imaging (MRI) is useful for differentiating ovarian tumors. In this review, we summarize the differential diagnoses for each of the five types of MRI findings commonly encountered in daily practice. First, unilocular cystic masses without mural nodules/solid components include benign lesions such as serous cystadenoma, functional cysts, surface epithelial inclusion cysts, paratubal cysts, and endometriosis. Second, multilocular cystic ovarian lesions include mucinous tumors and ovarian metastases. It should be noted that mucinous tumors may be diagnosed as borderline or carcinoma, even if no solid component is observed. Third, cystic lesions with mural nodules that are unrelated to endometriosis include serous borderline tumor and serous carcinoma. Cystic lesions with solid components are more likely to be malignant, but some may be diagnosed as benign. Fourth, ovarian tumors deriving from endometriosis include seromucinous borderline tumors, endometrioid carcinoma, and clear cell carcinoma. These tumors sometimes need to be differentiated from serous tumors. Finally, cystic lesions with lipid contents include teratoma-related tumors. In mature cystic teratoma, mural nodules (called "Rokitansky protuberance" or "dermoid nipple") are sometimes seen, but they do not suggest malignancy. Some of these lesions can be diagnosed accurately by considering their characteristic imaging findings, their changes over time, MRI findings other than those of the primary lesion, and information from other modalities such as tumor markers. To ensure the optimal treatment for ovarian tumors, it is important to estimate the histological type as well as to diagnose whether a lesion is benign or malignant.
Keywords: Cystic ovarian tumor; Differential diagnosis; Magnetic resonance imaging.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Cheung AN, Ellenson LH, Gilks CB, Kim K-R, Kong CS, Lax SF, et al. Tumours of the ovary. In: WHO Classification of Tumors Editorial Board. Female Genital Tumours 5th ed. Lyon: IARC Publications; 2020. p. 31–167.
-
- Oliva E (2020) Endometriosis and related conditions In: WHO classification of tumors Editorial Board. Female Genital Tumours. 5th ed. Lyon: IARC Publications; p. 169–173.
-
- Taylor EC, Irshaid L, Mathur M. Multimodality imaging approach to ovarian neoplasms with pathologic correlation. Radiographics. 2021;41:289–315. - PubMed
-
- Thomassin-Naggara I, Poncelet E, Jalaguier-Coudray A, Guerra A, Fournire LS, Stojanovic S, et al. Ovarian-Adnexal reporting data system magnetic resonance imaging (O-RADS MRI) score for risk stratification of Sonographically indeterminate adnexal masses. JAMA Netw Open. 2020;3:e1919896. doi: 10.1001/jamanetworkopen.2019.19896. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
