

Multimodality Imaging of Constrictive Pericarditis: Pathophysiology and New Concepts
- PMID: 35917048
- PMCID: PMC9344806
- DOI: 10.1007/s11886-022-01758-6
Multimodality Imaging of Constrictive Pericarditis: Pathophysiology and New Concepts
Abstract
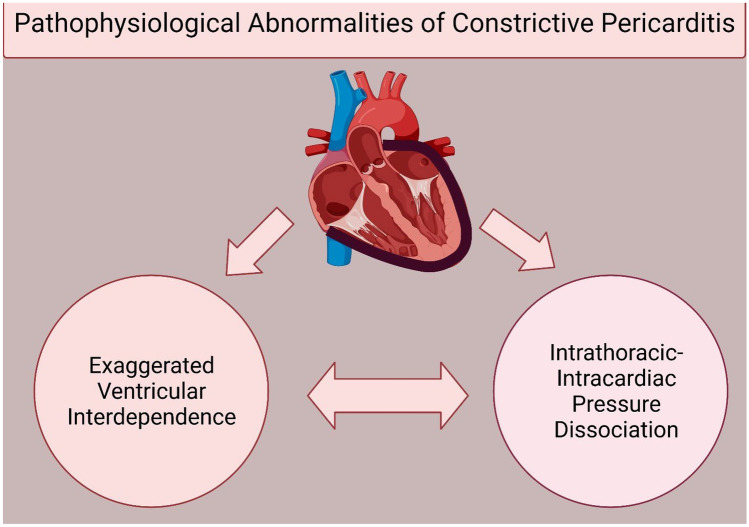
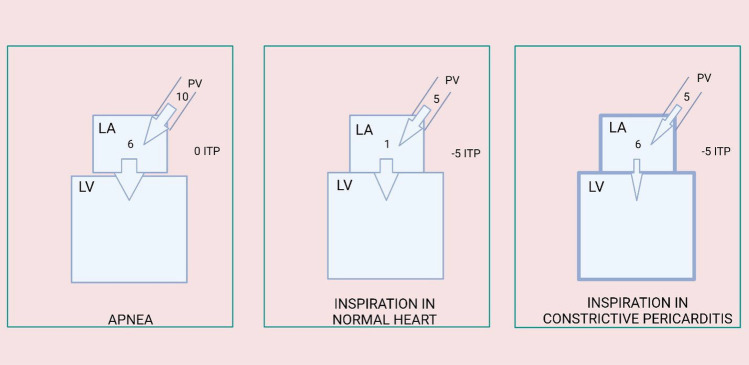
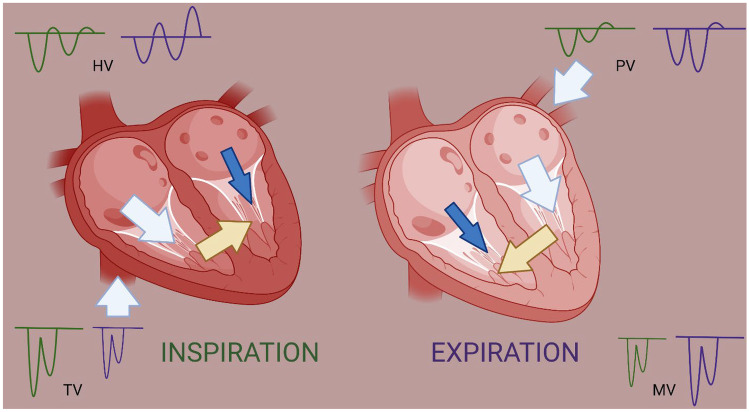
Purpose of review: The unique pathophysiological changes of constrictive pericarditis (CP) can now be identified with better imaging modalities, thereby helping in its early diagnosis. Through this review, we outline the pathophysiology of CP and its translation into symptomology and various imaging findings which then are used for both diagnosis and guiding treatment options for CP.
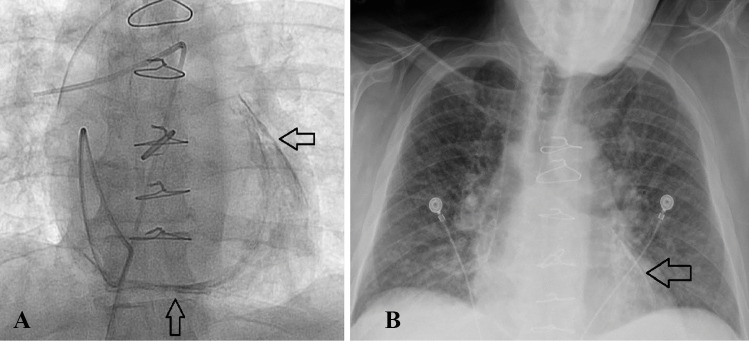
Recent findings: Multimodality imaging has provided us with the capability to recognize early stages of the disease and identify patients with a potential for reversibility and can be treated with medical management. Additionally, peri-procedural planning and prediction of post-operative complications has been made possible with the use of advanced imaging techniques. Advanced imaging has the potential to play a greater role in identification of patients with reversible disease process and provide peri-procedural risk stratification, thereby improving outcomes for patients with CP.
Keywords: Cardiac magnetic resonance imaging; Constrictive pericarditis; Multimodality imaging; Pathophysiology; Pre-operative imaging.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
The authors report no disclosures pertaining to this article.
Figures
References
-
- Brandt RR, Oh JK. Constrictive pericarditis: role of echocardiography and magnetic resonance imaging. E-Journal Cardiol Pract. 2017;15:22.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
