

Accuracy of CT perfusion ischemic core volume and location estimation: A comparison between four ischemic core estimation approaches using syngo.via
- PMID: 35917382
- PMCID: PMC9345340
- DOI: 10.1371/journal.pone.0272276
Accuracy of CT perfusion ischemic core volume and location estimation: A comparison between four ischemic core estimation approaches using syngo.via
Abstract
Background and objective: Computed tomography perfusion (CTP) is widely used in the evaluation of acute ischemic stroke patients for endovascular thrombectomy (EVT). The stability of CTP core estimation is suboptimal and varies between software packages. We aimed to quantify the volumetric and spatial agreement between the CTP ischemic core and follow-up infarct for four ischemic core estimation approaches using syngo.via.
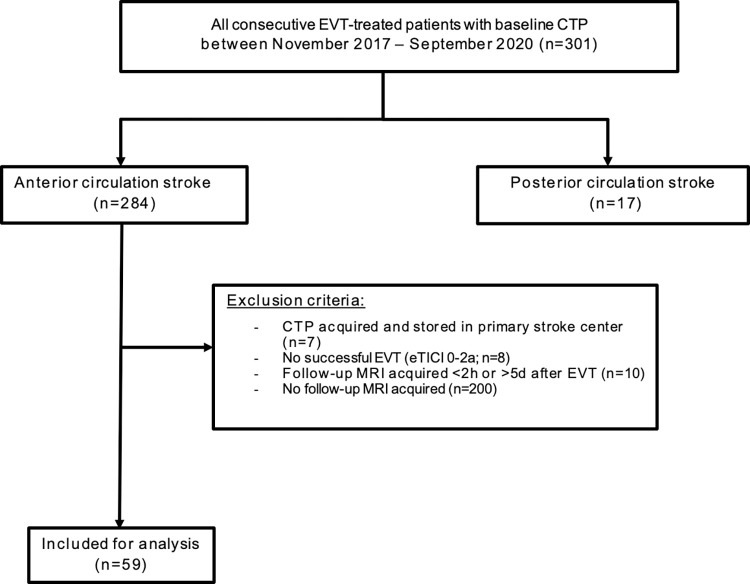
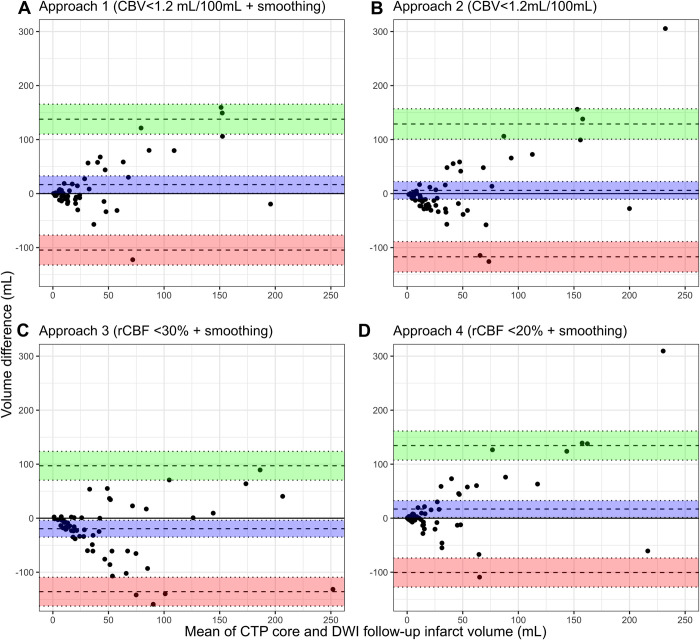
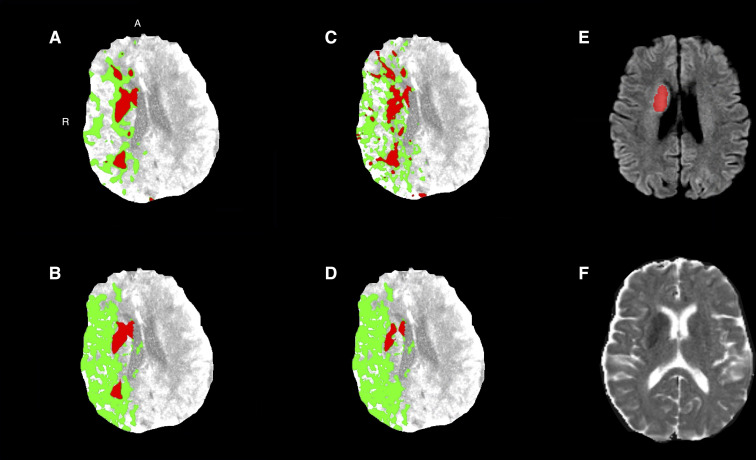
Methods: We included successfully reperfused, EVT-treated patients with baseline CTP and 24h follow-up diffusion weighted magnetic resonance imaging (DWI) (November 2017-September 2020). Data were processed with syngo.via VB40 using four core estimation approaches based on: cerebral blood volume (CBV)<1.2mL/100mL with and without smoothing filter, relative cerebral blood flow (rCBF)<30%, and rCBF<20%. The follow-up infarct was segmented on DWI.
Results: In 59 patients, median estimated CTP core volumes for four core estimation approaches ranged from 12-39 mL. Median 24h follow-up DWI infarct volume was 11 mL. The intraclass correlation coefficient (ICC) showed moderate-good volumetric agreement for all approaches (range 0.61-0.76). Median Dice was low for all approaches (range 0.16-0.21). CTP core overestimation >10mL occurred least frequent (14/59 [24%] patients) using the CBV-based core estimation approach with smoothing filter.
Conclusions: In successfully reperfused patients who underwent EVT, syngo.via CTP ischemic core estimation showed moderate volumetric and spatial agreement with the follow-up infarct on DWI. In patients with complete reperfusion after EVT, the volumetric agreement was excellent. A CTP core estimation approach based on CBV<1.2 mL/100mL with smoothing filter least often overestimated the follow-up infarct volume and is therefore preferred for clinical decision making using syngo.via.
Conflict of interest statement
We have read the journal’s policy and the authors of this manuscript have the following competing interests: HAM is co-founder and shareholder of Nicolab. BJE reports grants from Stryker Neurovascular and personal fees from Dekra and Novartis outside the submitted work. CBLMM is shareholder of Nicolab and reports grants from TWIN, CVON/Dutch Heart Foundation, and Stryker outside the submitted work. This does not alter our adherence to PLOS ONE policies on sharing data and materials. All other authors declare no support from any organization or financial relationships with any organizations that might have an interest in the submitted work. All authors declare no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Quantifying infarct core volume in ischemic stroke: What is the optimal threshold and parameters of computed tomography perfusion?J Stroke Cerebrovasc Dis. 2023 Jun;32(6):107062. doi: 10.1016/j.jstrokecerebrovasdis.2023.107062. Epub 2023 Mar 20. J Stroke Cerebrovasc Dis. 2023. PMID: 36948076
-
Volumetric and Spatial Accuracy of Computed Tomography Perfusion Estimated Ischemic Core Volume in Patients With Acute Ischemic Stroke.Stroke. 2018 Oct;49(10):2368-2375. doi: 10.1161/STROKEAHA.118.020846. Stroke. 2018. PMID: 30355095
-
Accuracy of CT Perfusion-Based Core Estimation of Follow-up Infarction: Effects of Time Since Last Known Well.Neurology. 2022 May 24;98(21):e2084-e2096. doi: 10.1212/WNL.0000000000200269. Epub 2022 Apr 21. Neurology. 2022. PMID: 35450966 Free PMC article.
-
Automated CT Perfusion Detection of the Acute Infarct Core in Ischemic Stroke: A Systematic Review and Meta-Analysis.Cerebrovasc Dis. 2023;52(1):97-109. doi: 10.1159/000524916. Epub 2022 Jun 3. Cerebrovasc Dis. 2023. PMID: 35661075
-
Application of Perfusion Imaging in the Telehealth Setting for Acute Ischemic Stroke.Acta Neurol Taiwan. 2024 Jun 30;33(2):37-46. Acta Neurol Taiwan. 2024. PMID: 39363420 Review.
Cited by
-
Agreement between estimated computed tomography perfusion ischemic core and follow-up infarct on diffusion-weighted imaging.Insights Imaging. 2022 Dec 13;13(1):191. doi: 10.1186/s13244-022-01334-0. Insights Imaging. 2022. PMID: 36512159 Free PMC article.
-
Role of artificial intelligence and machine learning in the diagnosis of cerebrovascular disease.Front Hum Neurosci. 2023 Sep 7;17:1254417. doi: 10.3389/fnhum.2023.1254417. eCollection 2023. Front Hum Neurosci. 2023. PMID: 37746051 Free PMC article. Review.
-
Accuracy of Four Different CT Perfusion Thresholds for Ischemic Core Volume and Location Estimation Using IntelliSpace Portal.J Cardiovasc Dev Dis. 2023 May 30;10(6):239. doi: 10.3390/jcdd10060239. J Cardiovasc Dev Dis. 2023. PMID: 37367404 Free PMC article.
-
Spatial accuracy of computed tomography perfusion to estimate the follow-up infarct on diffusion-weighted imaging after successful mechanical thrombectomy.BMC Neurol. 2023 Jan 20;23(1):31. doi: 10.1186/s12883-023-03075-z. BMC Neurol. 2023. PMID: 36670367 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
