

Advanced Techniques for Ethanol Ablation of Left Ventricular Summit Region Arrhythmias
- PMID: 35917467
- PMCID: PMC9388546
- DOI: 10.1161/CIRCEP.122.011017
Advanced Techniques for Ethanol Ablation of Left Ventricular Summit Region Arrhythmias
Abstract
Background: Coronary venous ethanol ablation (VEA) can be used as a strategy to treat ventricular arrhythmias arising from the left ventricular summit, but collateral flow and technical challenges cannulating intramural veins in complex venous anatomies can limit its use. Advanced techniques for VEA can capitalize on collateral vessels between target and nontarget sites to improve success.
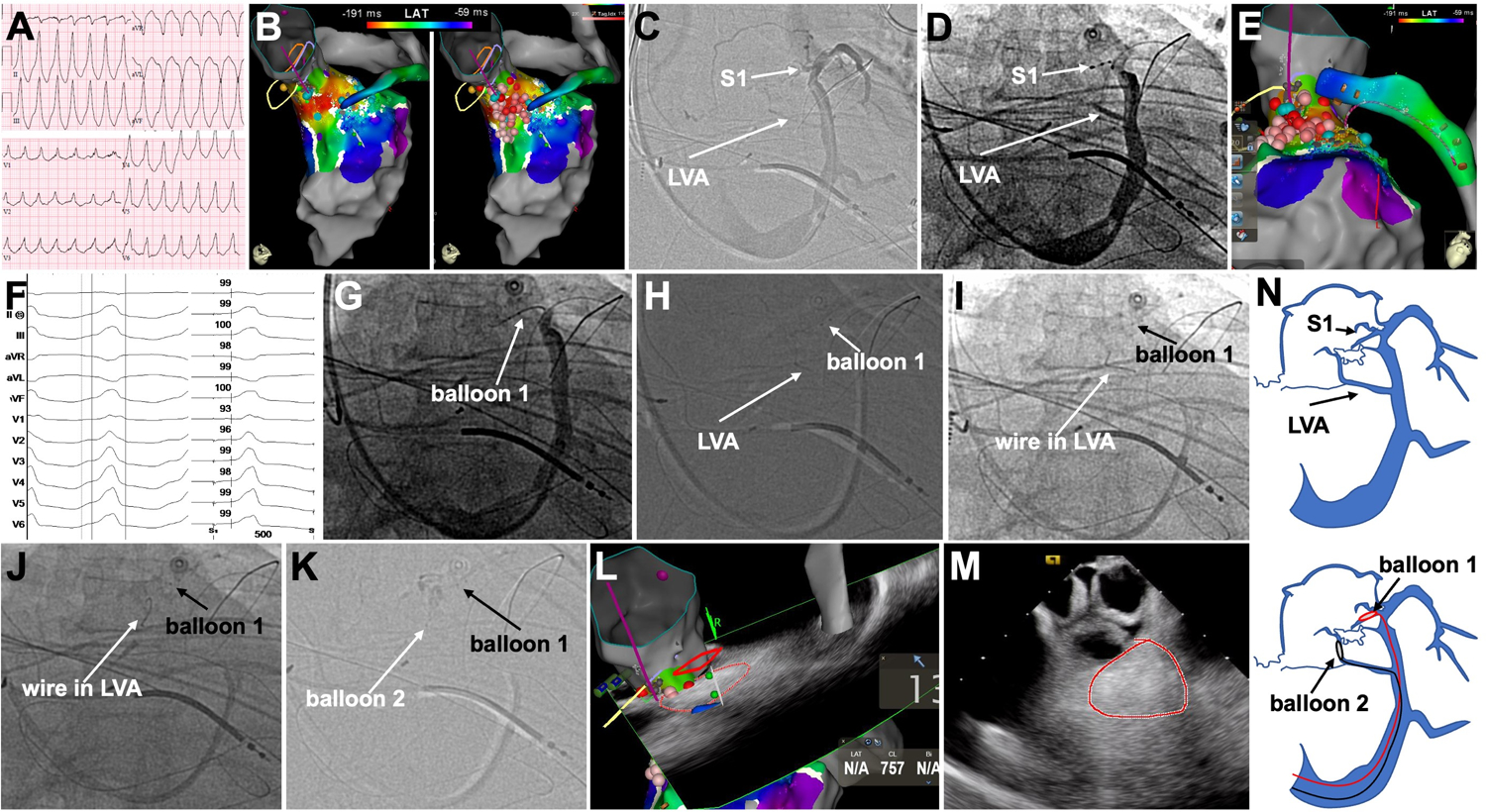
Methods: Of 55 patients with left ventricular summit ventricular arrhythmia, advanced techniques were used in 15 after initial left ventricular summit intramural vein mapping failed to show suitable targets for single vein, single-balloon VEA. All patients had previous radiofrequency ablation attempts. Techniques included: double-balloon for distal protection to block distal flow and target the proximal portion of a large intramural vein where best signal was proximal (n=6); balloons in 2 different left ventricular summit veins for a cross-fire multivein VEA (n=4); intramural collateral vein-to-vein cannulation to reach of targeted vein via collateral with antegrade ethanol and proximal balloon block (n=2); prolonged ethanol dwell time for vein sclerosis of large intramural vein and subsequent VEA (n=3); and intramural collateral VEA (n=1).
Results: Fifteen (8 females) patients (age 60.6±17.6 years) required advanced techniques. Procedure time was 210±49.9 minutes, fluoroscopy time was 25.3±14.1 minutes, and 113±17.9 cc of contrast was utilized. A median of 7 cc of ethanol was delivered (range, 4-15 cc). Intraprocedural radiofrequency ablation was delivered before ethanol in 9 out of 15 patients but failed. Ethanol achieved acute success in all 15 patients. Ethanol was used as the sole treatment in two patients. At a median follow-up of 194 days, one patient experienced recurrence.
Conclusions: Advanced techniques capitalizing on venous anatomy can enable successful VEA and selective targeting of arrhythmogenic sites, by blocking distal flow, utilization of collaterals between nontarget and target veins and multivein VEA. Understanding individual anatomy is critical for VEA success.
Keywords: catheter; coronary sinus; ethanol; sclerosis; veins.
Figures






References
-
- Tavares L, Valderrábano M. Retrograde venous ethanol ablation for ventricular tachycardia. Heart Rhythm. 2019;16(3):478–483. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
