

Imaging the neural underpinnings of freezing of gait in Parkinson's disease
- PMID: 35917720
- PMCID: PMC9421505
- DOI: 10.1016/j.nicl.2022.103123
Imaging the neural underpinnings of freezing of gait in Parkinson's disease
Abstract
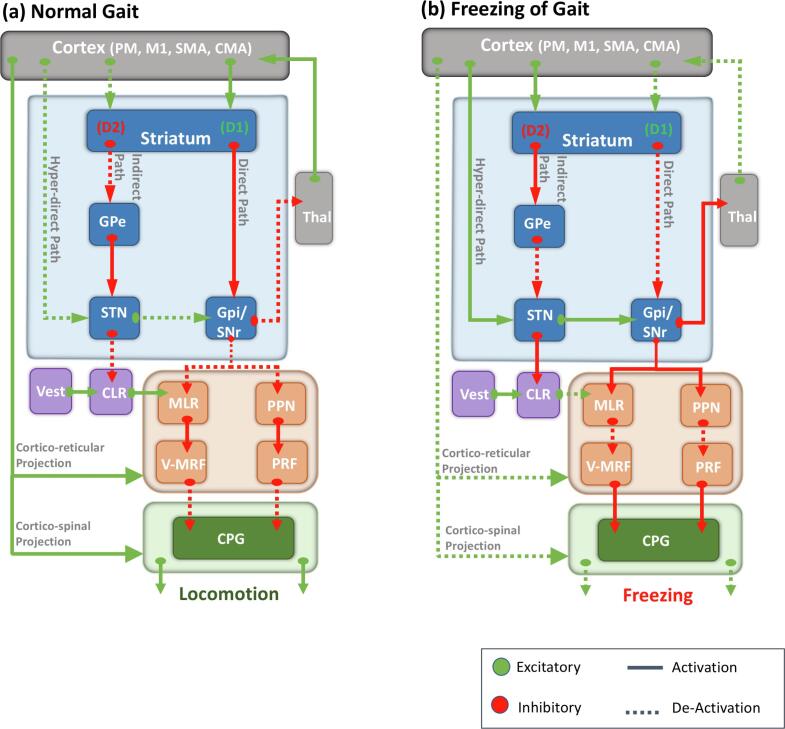
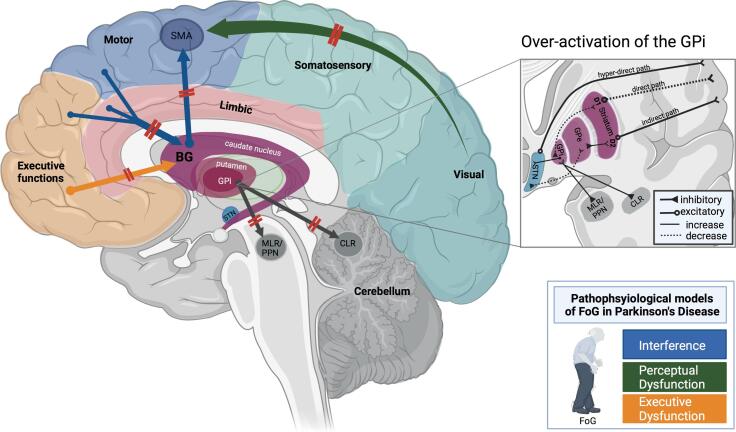
Freezing of gait (FoG) is a paroxysmal and sporadic gait impairment that severely affects PD patients' quality of life. This review summarizes current neuroimaging investigations that characterize the neural underpinnings of FoG in PD. The review presents and discusses the latest advances across multiple methodological domains that shed light on structural correlates, connectivity changes, and activation patterns associated with the different pathophysiological models of FoG in PD. Resting-state fMRI studies mainly report cortico-striatal decoupling and disruptions in connectivity along the dorsal stream of visuomotor processing, thus supporting the 'interference' and the 'perceptual dysfunction' models of FoG. Task-based MRI studies employing virtual reality and motor imagery paradigms reveal a disruption in functional connectivity between cortical and subcortical regions and an increased recruitment of parieto-occipital regions, thus corroborating the 'interference' and 'perceptual dysfunction' models of FoG. The main findings of fNIRS studies of actual gait primarily reveal increased recruitment of frontal areas during gait, supporting the 'executive dysfunction' model of FoG. Finally, we discuss how identifying the neural substrates of FoG may open new avenues to develop efficient treatment strategies.
Keywords: Gait impairment; Locomotor regions; Motor imagery; Neuroimaging; Virtual reality.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Alterations of functional and structural connectivity of freezing of gait in Parkinson's disease.J Neurol. 2016 Aug;263(8):1583-92. doi: 10.1007/s00415-016-8174-4. Epub 2016 May 26. J Neurol. 2016. PMID: 27230857
-
Functional MRI in Parkinson's disease with freezing of gait: a systematic review of the literature.Neurol Sci. 2021 May;42(5):1759-1771. doi: 10.1007/s10072-021-05121-5. Epub 2021 Mar 13. Neurol Sci. 2021. PMID: 33713258
-
Lateralized Connectivity between Globus Pallidus and Motor Cortex is Associated with Freezing of Gait in Parkinson's Disease.Neuroscience. 2020 Sep 1;443:44-58. doi: 10.1016/j.neuroscience.2020.06.036. Epub 2020 Jul 3. Neuroscience. 2020. PMID: 32629155 Free PMC article.
-
Freezing of gait in Parkinson's disease is associated with altered functional brain connectivity.Parkinsonism Relat Disord. 2016 Mar;24:100-6. doi: 10.1016/j.parkreldis.2015.12.016. Epub 2015 Dec 30. Parkinsonism Relat Disord. 2016. PMID: 26776567
-
Neuroimaging advances in Parkinson's disease with freezing of gait: A systematic review.Neuroimage Clin. 2019;24:102059. doi: 10.1016/j.nicl.2019.102059. Epub 2019 Nov 9. Neuroimage Clin. 2019. PMID: 31795038 Free PMC article.
Cited by
-
Triggers for freezing of gait in individuals with Parkinson's disease: a systematic review.Front Neurol. 2023 Dec 21;14:1326300. doi: 10.3389/fneur.2023.1326300. eCollection 2023. Front Neurol. 2023. PMID: 38187152 Free PMC article. Review.
-
Management of freezing of gait - mechanism-based practical recommendations.Nat Rev Neurol. 2025 Jun;21(6):327-344. doi: 10.1038/s41582-025-01079-6. Epub 2025 Apr 1. Nat Rev Neurol. 2025. PMID: 40169855 Review.
-
Atrophy of ventral diencephalon is associated with freezing of gait in Parkinson's disease: analysis of two cohorts.NPJ Parkinsons Dis. 2025 Mar 6;11(1):44. doi: 10.1038/s41531-025-00893-5. NPJ Parkinsons Dis. 2025. PMID: 40050652 Free PMC article.
-
Efficacy of exercise interventions combined with Selegiline in ameliorating freezing of gait in Parkinson's disease patients.Am J Transl Res. 2024 Jul 15;16(7):2852-2863. doi: 10.62347/JTRH2408. eCollection 2024. Am J Transl Res. 2024. PMID: 39114711 Free PMC article.
-
Cholinergic system correlates of postural control changes in Parkinson's disease freezers.Brain. 2023 Aug 1;146(8):3243-3257. doi: 10.1093/brain/awad134. Brain. 2023. PMID: 37086478 Free PMC article.
References
-
- Amboni M., Stocchi F., Abruzzesse G., Morgante L., Onofri M., Ruggieri S., Tinazzi M., Sappia M., Attar M., Colombo D., Simoni L., Ori A., Barone P., Antonini A. Prevalence and associated features of self-reported freezing of gait in Parkinson’s disease: the DEEP FOG study. Park. Relat. Disord. 2015;21:644–649. - PubMed
-
- Azulay J.-P., Mesure S., Blin O. Influence of visual cues on gait in Parkinson’s disease: contribution to attention or sensory dependence? J. Neurol. Sci. 2006;248(1-2):192–195. - PubMed
-
- Barbe M.T., Amarell M., Snijders A.H., Florin E., Quatuor E.-L., Schönau E., Fink G.R., Bloem B.R., Timmermann L. Gait and upper limb variability in Parkinson’s disease patients with and without freezing of gait. J. Neurol. 2014;261(2):330–342. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
