

Intraoperative fluid balance and cardiac surgery-associated acute kidney injury: a multicenter prospective study
- PMID: 35917847
- PMCID: PMC9659999
- DOI: 10.1016/j.bjane.2022.07.006
Intraoperative fluid balance and cardiac surgery-associated acute kidney injury: a multicenter prospective study
Abstract
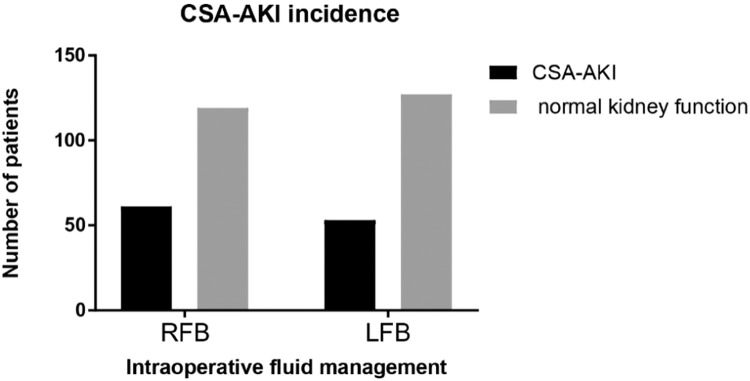
Background: Recent data suggest the regime of fluid therapy intraoperatively in patients undergoing major surgeries may interfere in patient outcomes. The development of postoperative Acute Kidney Injury (AKI) has been associated with both Restrictive Fluid Balance (RFB) and Liberal Fluid Balance (LFB) during non-cardiac surgery. In patients undergoing cardiac surgery, this influence remains unclear. The study objective was to evaluate the relationship between intraoperative RFB vs. LFB and the incidence of Cardiac-Surgery-Associated AKI (CSA-AKI) and major postoperative outcomes in patients undergoing on-pump Coronary Artery Bypass Grafting (CABG).
Methods: This prospective, multicenter, observational cohort study was set at two high-complexity university hospitals in Brazil. Adult patients who required postoperative intensive care after undergoing elective on-pump CABG were allocated to two groups according to their intraoperative fluid strategy (RFB or LFB) with no intervention.
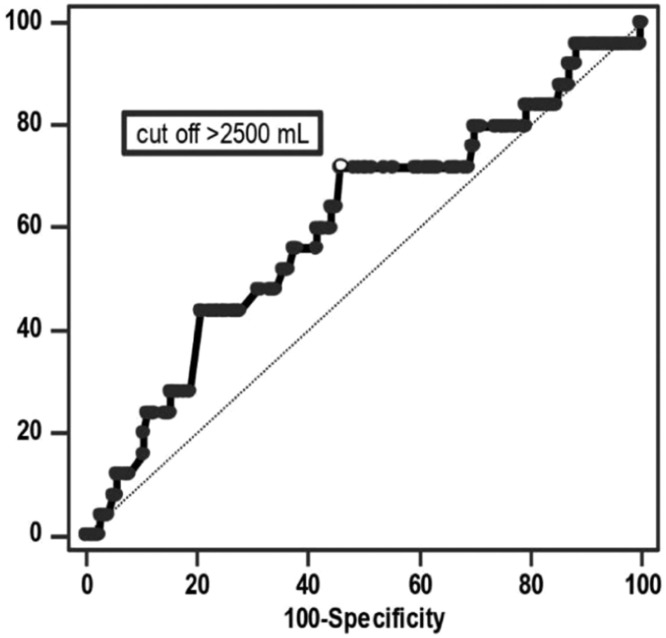
Results: The primary endpoint was CSA-AKI. The secondary outcomes were in-hospital mortality, cardiovascular complications, ICU Length of Stay (ICU-LOS), and Hospital LOS (H-LOS). After propensity score matching, 180 patients remained in each group. There was no difference in risk of CSA-AKI between the two groups (RR = 1.15; 95% CI, 0.85-1.56, p = 0.36). The in-hospital mortality, H-LOS and cardiovascular complications were higher in the LFB group. ICU-LOS was not significantly different between the two groups. ROCcurve analysis determined a fluid balance above 2500 mL to accurately predict in-hospital mortality.
Conclusion: Patients undergoing on-pump CABG with LFB when compared with patients with RFB present similar CSA-AKI rates and ICU-LOS, but higher in-hospital mortality, cardiovascular complications, and H-LOS.
Keywords: Acute kidney injury; Cardiac surgery; Cardiopulmonary bypass; Cardiovascular disease; Coronary artery bypass; Fluid therapy.
Copyright © 2022 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. All rights reserved.
Conflict of interest statement
Conflicts of interest The authors declare no conflicts of interest.
Figures



References
-
- Nelson M, Green J, Spiess B, et al. Measurement of blood loss in cardiac surgery: still too much. Ann Thorac Surg. 2018;105:1176–1181. - PubMed
-
- Miller TE, Myles PS. Perioperative fluid therapy for major surgery. Anesthesiology. 2019;130:825–832. - PubMed
-
- Corredor C, Thomson R, Al-Subaie N. Long-Term Consequences of acute kidney injury after cardiac surgery: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth. 2016;30:69–75. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
