

Epidemiology, outcomes and predictors of mortality in patients transported by ambulance for dyspnoea: A population-based cohort study
- PMID: 35918062
- PMCID: PMC10947453
- DOI: 10.1111/1742-6723.14053
Epidemiology, outcomes and predictors of mortality in patients transported by ambulance for dyspnoea: A population-based cohort study
Abstract
Objectives: There are currently limited data to inform the management of patients transported by emergency medical services (EMS) with dyspnoea. We aimed to describe the incidence, aetiology and outcomes of patients transported by EMS for dyspnoea using a large population-based sample and to identify factors associated with 30-day mortality.
Methods: Consecutive EMS attendances for dyspnoea in Victoria, Australia from January 2015 to June 2019 were included. Data were individually linked to hospital and mortality records to determine incidence, diagnoses, and outcomes. Factors associated with 30-day mortality were assessed using multivariable logistic regression.
Results: During the study period, there were 2 505 324 cases attended by EMS, of whom 346 228 (14%) met inclusion criteria for dyspnoea. The incidence of EMS attendances for dyspnoea was 1566 per 100 000 person-years, and was higher in females, older patients and socially disadvantaged areas. Of the 271 204 successfully linked cases (median age 76 years; 51% women), 79% required hospital admission with a 30-day mortality of 9%. The most common final diagnoses (and 30-day mortality rates) were lower respiratory tract infection (13%, mortality 11%), chronic obstructive pulmonary disease (13%, mortality 6.4%), heart failure (9.1%, mortality 9.8%), arrhythmias (3.9%, mortality 4.4%), acute coronary syndromes (3.9%, mortality 9.5%) and asthma (3.2%, mortality 0.5%). Predictors of mortality included older age, male sex, pre-existing chronic kidney disease, heart failure or cancer, abnormal respiratory status or vital signs and pre-hospital intubation.
Conclusion: Dyspnoea is a common presentation with a broad range of causes and is associated with high rates of hospitalisation and death.
Keywords: ambulance; dyspnoea; emergency medicine; epidemiology; shortness of breath.
© 2022 The Authors. Emergency Medicine Australasia published by John Wiley & Sons Australia, Ltd on behalf of Australasian College for Emergency Medicine.
Conflict of interest statement
None declared.
Figures
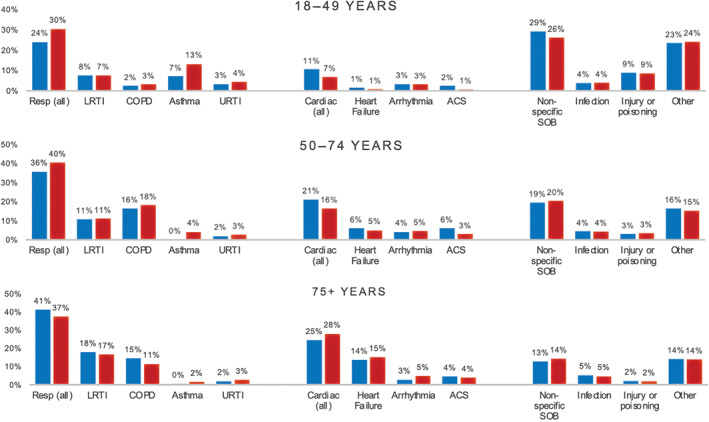
 indicates male,
indicates male,  indicates female). ACS, acute coronary syndromes; COPD, chronic obstructive pulmonary disease; LRTI, lower respiratory tract infection; SOB, shortness of breath; URTI, upper respiratory tract infection.
indicates female). ACS, acute coronary syndromes; COPD, chronic obstructive pulmonary disease; LRTI, lower respiratory tract infection; SOB, shortness of breath; URTI, upper respiratory tract infection.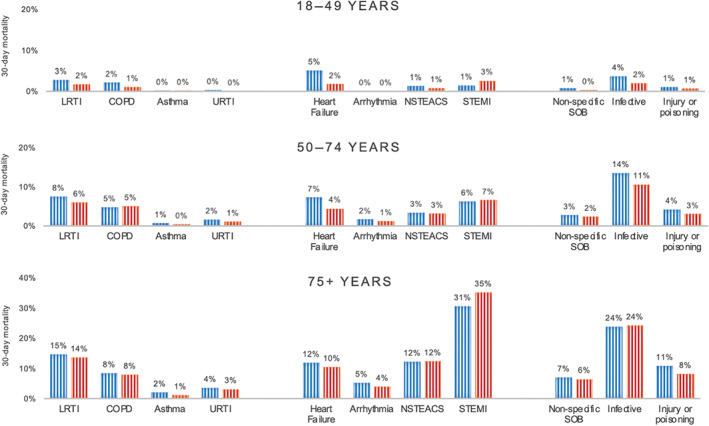
 indicates male,
indicates male,  indicates female). COPD, chronic obstructive pulmonary disease; LRTI, lower respiratory tract infection; NSTEACS, non ST‐elevation myocardial infarction; STEMI, ST elevation myocardial infarction; URTI, upper respiratory tract infection.
indicates female). COPD, chronic obstructive pulmonary disease; LRTI, lower respiratory tract infection; NSTEACS, non ST‐elevation myocardial infarction; STEMI, ST elevation myocardial infarction; URTI, upper respiratory tract infection.Similar articles
-
Impact of socioeconomic status on presentation, care quality and outcomes of patients attended by emergency medical services for dyspnoea: a population-based cohort study.J Epidemiol Community Health. 2024 Mar 8;78(4):255-262. doi: 10.1136/jech-2023-220737. J Epidemiol Community Health. 2024. PMID: 38228390
-
Incidence and Outcomes of Nontraumatic Shock in Adults Using Emergency Medical Services in Victoria, Australia.JAMA Netw Open. 2022 Jan 4;5(1):e2145179. doi: 10.1001/jamanetworkopen.2021.45179. JAMA Netw Open. 2022. PMID: 35080603 Free PMC article.
-
Incidence, diagnoses and outcomes of ambulance attendances for chest pain: a population-based cohort study.Ann Epidemiol. 2022 Aug;72:32-39. doi: 10.1016/j.annepidem.2022.04.010. Epub 2022 May 2. Ann Epidemiol. 2022. PMID: 35513303
-
The epidemiology of elderly falls attended by emergency medical services in Victoria, Australia.Injury. 2018 Sep;49(9):1712-1719. doi: 10.1016/j.injury.2018.06.038. Epub 2018 Jun 25. Injury. 2018. PMID: 30126534
-
Pre-hospital predictors of an adverse outcome among patients with dyspnoea as the main symptom assessed by pre-hospital emergency nurses - a retrospective observational study.BMC Emerg Med. 2020 Nov 10;20(1):89. doi: 10.1186/s12873-020-00384-1. BMC Emerg Med. 2020. PMID: 33172409 Free PMC article.
Cited by
-
Breathlessness intensity recorded in general practice is associated with shorter times to unplanned hospital admissions and longer lengths of stay: a UK cohort study.BMJ Open Respir Res. 2025 Jul 30;12(1):e003000. doi: 10.1136/bmjresp-2024-003000. BMJ Open Respir Res. 2025. PMID: 40738555 Free PMC article.
-
Prognosis of patients with nonspecific electrocardiogram findings in a Tanzanian emergency department.Am Heart J. 2025 Mar;281:10-19. doi: 10.1016/j.ahj.2024.11.006. Epub 2024 Dec 19. Am Heart J. 2025. PMID: 39577681
-
Prehospital critical care drug-therapy and 30-day mortality in patients with acute respiratory disease.World J Emerg Med. 2025;16(1):43-50. doi: 10.5847/wjem.j.1920-8642.2025.008. World J Emerg Med. 2025. PMID: 39906107 Free PMC article.
-
Prevalence and Economic Impact of Acute Respiratory Failure in the Prehospital Emergency Medical Service of the Madrid Community: Retrospective Cohort Study.JMIR Public Health Surveill. 2025 Jan 16;11:e66179. doi: 10.2196/66179. JMIR Public Health Surveill. 2025. PMID: 39819841 Free PMC article.
-
Prehospital Performance of Five Early Warning Scores to Predict Long-Term Mortality in Patients with Suspected Respiratory Infections.Diagnostics (Basel). 2025 Jun 19;15(12):1565. doi: 10.3390/diagnostics15121565. Diagnostics (Basel). 2025. PMID: 40564885 Free PMC article.
References
-
- Kelly AM, Keijzers G, Klim S et al. An observational study of dyspnea in emergency departments: the Asia, Australia, and New Zealand dyspnea in emergency departments study (AANZDEM). Acad. Emerg. Med. 2017; 24: 328–36. - PubMed
-
- Nehme Z, Bernard S, Cameron P et al. Using a cardiac arrest registry to measure the quality of emergency medical service care: decade of findings from the Victorian ambulance cardiac arrest registry. Circ. Cardiovasc. Qual. Outcomes 2015; 8: 56–66. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
