

Flow diversion for compressive unruptured internal carotid artery aneurysms with neuro-ophthalmological symptoms: a systematic review and meta-analysis
- PMID: 35918130
- PMCID: PMC10447391
- DOI: 10.1136/jnis-2022-019249
Flow diversion for compressive unruptured internal carotid artery aneurysms with neuro-ophthalmological symptoms: a systematic review and meta-analysis
Abstract
Background: Data on the safety and efficacy of flow diverters (FD) for the treatment of unruptured internal carotid artery (ICA) aneurysms with compressive neuro-ophthalmological symptoms (NOS) are scarce and comprise mainly small case series.
Methods: We performed a search of three databases and included series with ≥10 patients, with unruptured aneurysms of the ICA and NOS, treated with FD. Random-effects analysis of treatment results and safety was performed.
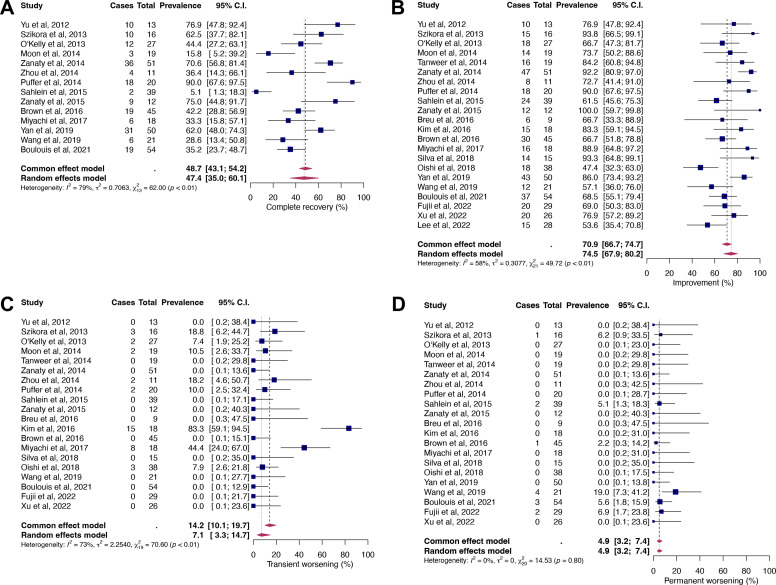
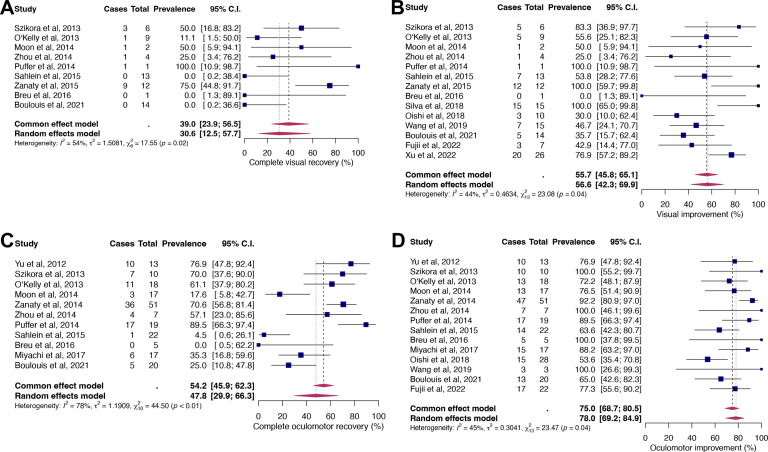
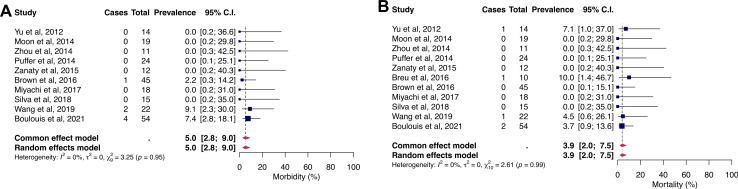
Results: A total of 22 studies reporting on 594 patients were included. Pooled proportions of NOS recovery, improvement, transient and permanent worsening were: 47.4% (95% CI 35.0% to 60.1%); 74.5% (95% CI 67.9% to 80.2%); 7.1% (95% CI 3.3% to 14.7%); and 4.9% (95% CI 3.2% to 7.4%), respectively. Rates of complete recovery and improvement in patients with isolated visual symptoms were 30.6% (95% CI 12.5% to 57.7%) and 56.6% (95% CI 42.3% to 69.9%). Isolated oculomotor symptoms recovered completely in 47.8% (95% CI 29.9% to 66.3%) and improved in 78% (95% CI 69.2% to 84.9%). Morbidity occurred in 5% (95% CI 2.8% to 9%) and mortality in 3.9% (95% CI 2% to 7.5%) of patients. An increased likelihood of symptom improvement was observed when treatment was performed early (<1 month) after symptom onset (OR=11.22, 95% CI 3.9% to 32.5%).
Conclusion: Flow diversion promotes recovery or improvement of compressive symptoms in a large proportion of patients but is associated with significant rates of morbidity and mortality. Transient and permanent NOS worsening is not uncommon. Early treatment is of utmost importance, as it increases the likelihood of symptom improvement more than 10-fold.
Keywords: Aneurysm; Complication; Flow Diverter; Stent.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: DPOK: Received stents from Phenox for research purposes and funding from the Else Körner Fresenius Center of Digital Health and the Joachim Herz Foundation; has a non-financial research agreement with Brainomix; serves as board member of the German Society of Neuroradiology (DGNR). MG: Consultancy contract with Phenox; proctoring contract with MicroVention; member of the clinical event committee for a study on a flow diverter, sponsored by Microvention; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events by Phenox; received stents from Phenox for research purposes; received funding from the Else Körner Fresenius Center of Digital Health.
Figures

Similar articles
-
Flow diversion for internal carotid artery aneurysms with compressive neuro-ophthalmologic symptoms: clinical and anatomical results in an international multicenter study.J Neurointerv Surg. 2022 Nov;14(11):1090-1095. doi: 10.1136/neurintsurg-2021-018188. Epub 2021 Nov 18. J Neurointerv Surg. 2022. PMID: 34795018
-
Onset-to-treatment time and aneurysmal regression predict improvement of cranial neuropathy after flow diversion treatment in patients with symptomatic internal carotid artery aneurysms.J Neurointerv Surg. 2023 Sep;15(9):886-891. doi: 10.1136/jnis-2022-019202. Epub 2022 Jul 19. J Neurointerv Surg. 2023. PMID: 35853697 Free PMC article.
-
Mass Effect After Flow Diversion for Unruptured Large and Giant Cavernous or Paraclinoid Internal Carotid Artery Aneurysm.World Neurosurg. 2023 Dec;180:e108-e116. doi: 10.1016/j.wneu.2023.08.129. Epub 2023 Sep 9. World Neurosurg. 2023. PMID: 37690582
-
A rare but morbid neurosurgical target: petrous aneurysms and their endovascular management in the stent/flow diverter era.J Neurointerv Surg. 2017 Apr;9(4):381-383. doi: 10.1136/neurintsurg-2016-012668. Epub 2016 Sep 26. J Neurointerv Surg. 2017. PMID: 27672098 Review.
-
Flow-Diverter Stent for an Unruptured Aneurysm at the Junction of the Internal Carotid Artery and Persistent Primitive Trigeminal Artery: Case Report and Literature Review.World Neurosurg. 2019 Dec;132:329-332. doi: 10.1016/j.wneu.2019.08.199. Epub 2019 Sep 5. World Neurosurg. 2019. PMID: 31493612 Review.
Cited by
-
An overview of decision-making in cerebrovascular treatment strategies: Part I - unruptured aneurysms.Brain Spine. 2024 Sep 5;4:103331. doi: 10.1016/j.bas.2024.103331. eCollection 2024. Brain Spine. 2024. PMID: 39309547 Free PMC article. Review.
-
Systematic evaluation of neuro-ophthalmic outcomes of the ophthalmic artery covered by flow-diverter.Front Neurol. 2025 Mar 18;16:1479229. doi: 10.3389/fneur.2025.1479229. eCollection 2025. Front Neurol. 2025. PMID: 40170895 Free PMC article. Review.
References
-
- van Rooij WJ, Sluzewski M. Unruptured large and giant carotid artery aneurysms presenting with cranial nerve palsy: comparison of clinical recovery after selective aneurysm coiling and therapeutic carotid artery occlusion. AJNR Am J Neuroradiol 2008;29:997–1002. 10.3174/ajnr.A1023 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous