

Reversal of collateral ventilation using endoscopic polymer foam in COPD patients undergoing endoscopic lung volume reduction with endobronchial valves: A controlled parallel group trial
- PMID: 35918295
- PMCID: PMC9804936
- DOI: 10.1111/resp.14338
Reversal of collateral ventilation using endoscopic polymer foam in COPD patients undergoing endoscopic lung volume reduction with endobronchial valves: A controlled parallel group trial
Abstract
Background and objective: We have previously described reversal of collateral ventilation (CV) in a severe chronic obstructive pulmonary disease (COPD) patient with endoscopic polymer foam (EPF), prior to endoscopic lung volume reduction (ELVR) with valves. The aim of this study was to investigate the efficacy of this in a larger cohort and compare outcomes with a similar cohort with no CV.
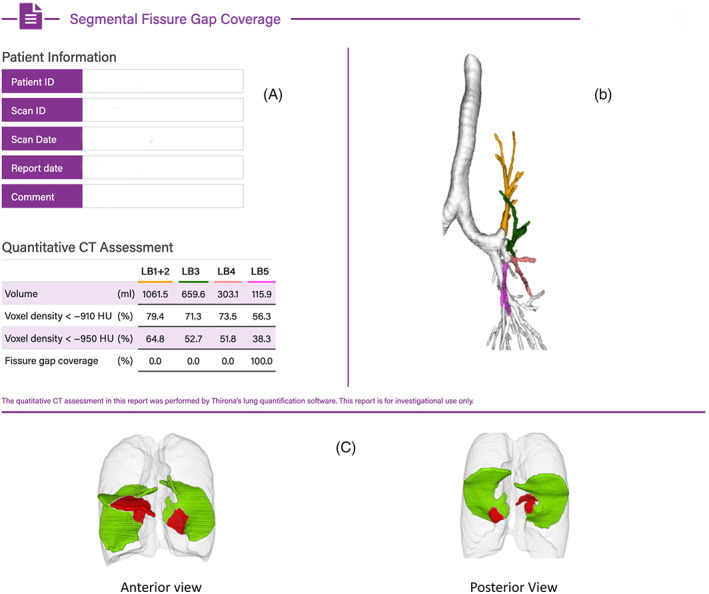
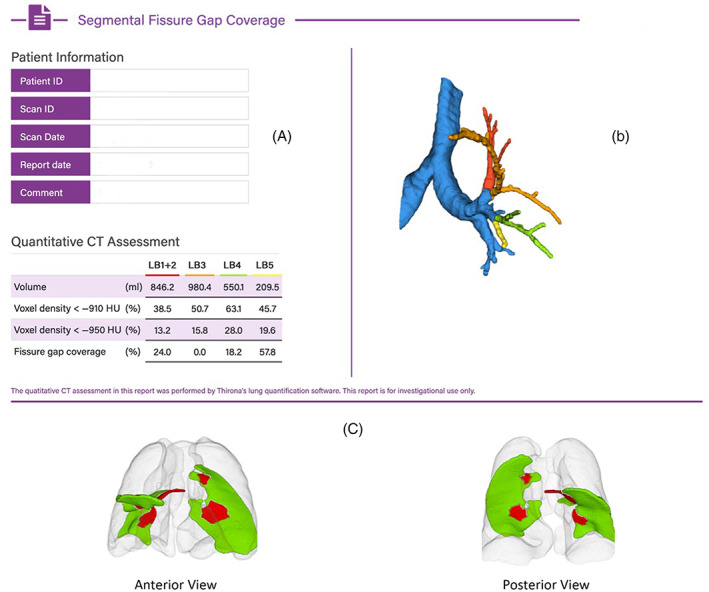
Methods: Patients with severe COPD, with the left upper lobe (LUL) targeted for ELVR, were assessed for CV with high resolution computed tomography (HRCT). If fissure completeness was >95% they were enrolled as controls for valves alone (endobronchial valve control group [EBV-CTRL]). If fissure completeness was 80%-95%, defects were mapped to the corresponding segment, where EPF was instilled following confirmation of CV with CHARTIS. EBVs were inserted 1 month afterwards.
Results: Fourteen patients were enrolled into both arms. After 6 months, there were significant improvements in both groups in forced expiratory volume in 1 s (FEV1; +19.7% EPF vs. +27.7% EBV-CTRL, p < 0.05); residual volume (RV; -16.2% EPF vs. -20.1% EBV-CTRL, p = NS); SGRQ (-15.1 EPF vs. -16.6 EBV-CTRL p = NS) and 6 min walk (+25.8% EPF [77.2 m] vs. +28.4% [82.3 m] EBV-CTRL p = NS). Patients with fissural defects mapped to the lingula had better outcomes than those mapped to other segments (FEV1 +22.9% vs. +16.3% p < 0.05). There were no serious adverse reactions to EPF.
Conclusion: EPF successfully reverses CV in severe COPD patients with a left oblique fissure that is 80%-95% complete. Following EBV, outcomes are similar to patients with complete fissures undergoing ELVR with EBV alone. EPF therapy to reverse CV potentially increases the number of COPD patients suitable for ELVR with minimal adverse reactions.
Trial registration: ClinicalTrials.gov NCT05396131.
Keywords: COPD; bronchoscopy and interventional techniques; chronic obstructive pulmonary disease; collateral ventilation; endobronchial valve; endoscopic lung volume reduction; polymer foam.
© 2022 The Authors. Respirology published by John Wiley & Sons Australia, Ltd on behalf of Asian Pacific Society of Respirology.
Conflict of interest statement
This is an investigator‐initiated trial funded by Pulmonx Australia. Alvin J. Ing has received consultancy fees in the past from Pulmonx Australia, Olympus Australia and Morair Medical. The other authors have made no disclosures.
Figures
Comment in
-
Sealing the gap in bronchoscopic lung volume reduction.Respirology. 2022 Dec;27(12):1012-1014. doi: 10.1111/resp.14371. Epub 2022 Sep 14. Respirology. 2022. PMID: 36104311 No abstract available.
References
-
- GOLD . 2020. Global Strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (2020 report). www.goldcopd.org
-
- Koster DT, van Rikxoort EM, Huebner RH, Doellinger F, Klooster K, Charbonnier JP, et al. Predicting lung volume reduction after endobronchial valve therapy is maximized using a combination of diagnostic tools. Respiration. 2016;92(3):150–7. - PubMed
-
- Carew A, Williamson JP, Philips MJ, Saghaie T, Garah CS, Ing AJ. Interventional bronchoscopy for chronic obstructive pulmonary disease: more than a pipe dream. Med J Aust. 2021;215(6):280–5. - PubMed
-
- Herth FJF, Slebos DJ, Criner GJ, Valipour A, Sciurba F, Shah PL. Endoscopic lung volume reduction: an expert panel recommendation—update 2019. Respiration. 2019;97:548–57. - PubMed
-
- Herth FJ, Gompelmann D, Stanzel F, Bonnet R, Behr J, Schmidt B, et al. Treatment of advanced emphysema with emphysematous lung sealant (AeriSeal®). Respiration. 2011;82:36–45. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
