

Construction of a novel signature and prediction of the immune landscape in gastric cancer based on necroptosis-related genes
- PMID: 35918354
- PMCID: PMC9345982
- DOI: 10.1038/s41598-022-15854-8
Construction of a novel signature and prediction of the immune landscape in gastric cancer based on necroptosis-related genes
Abstract
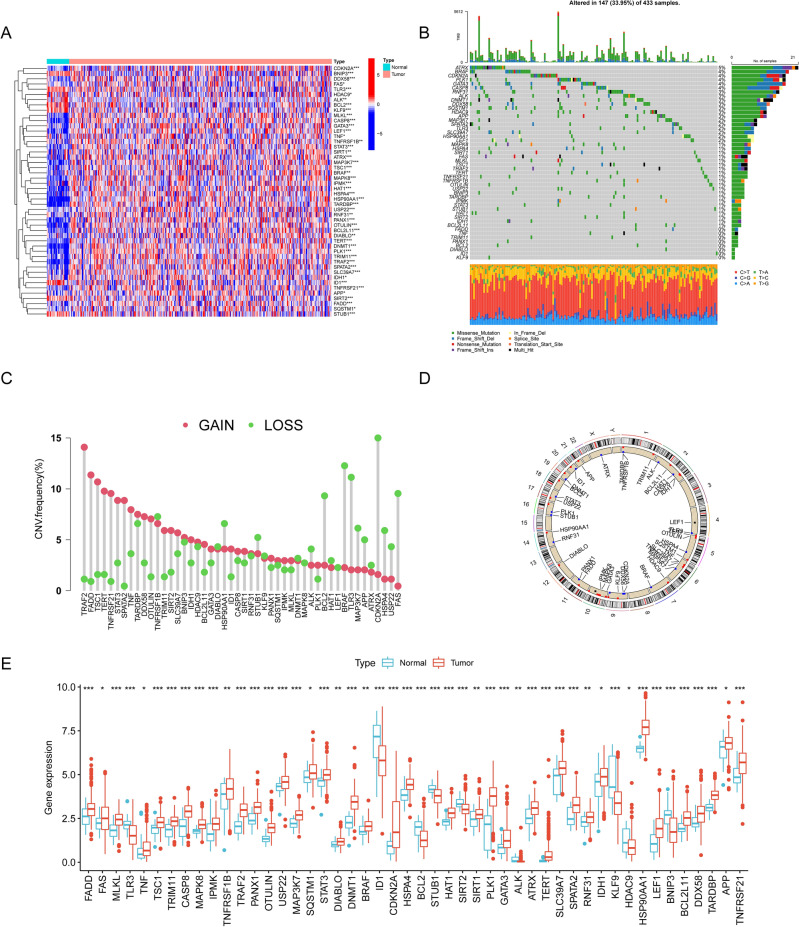
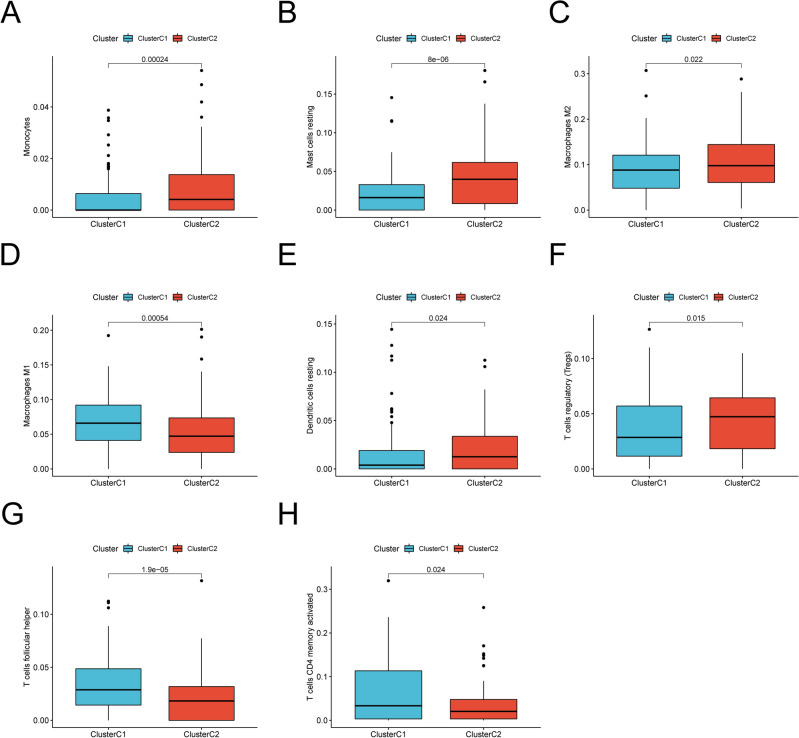
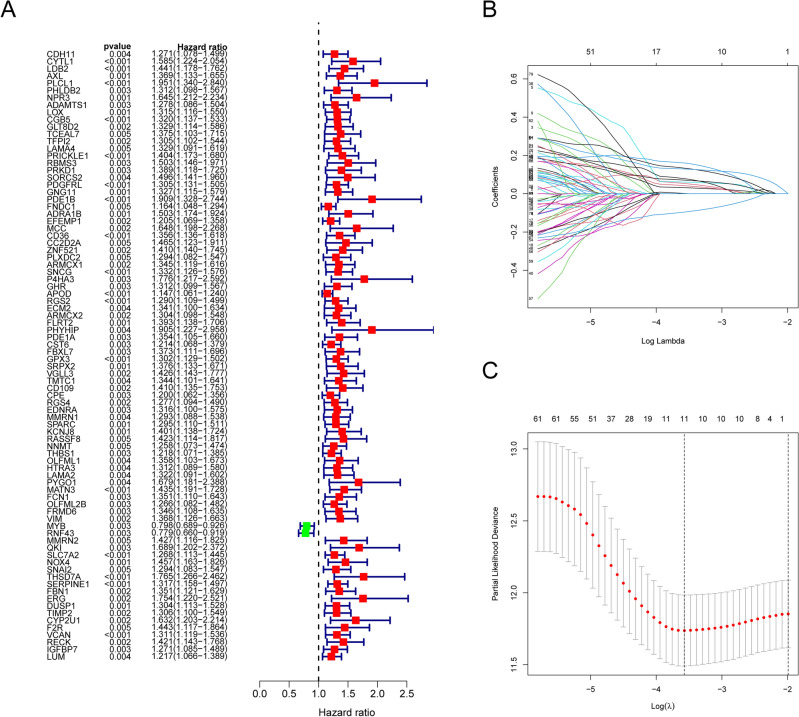
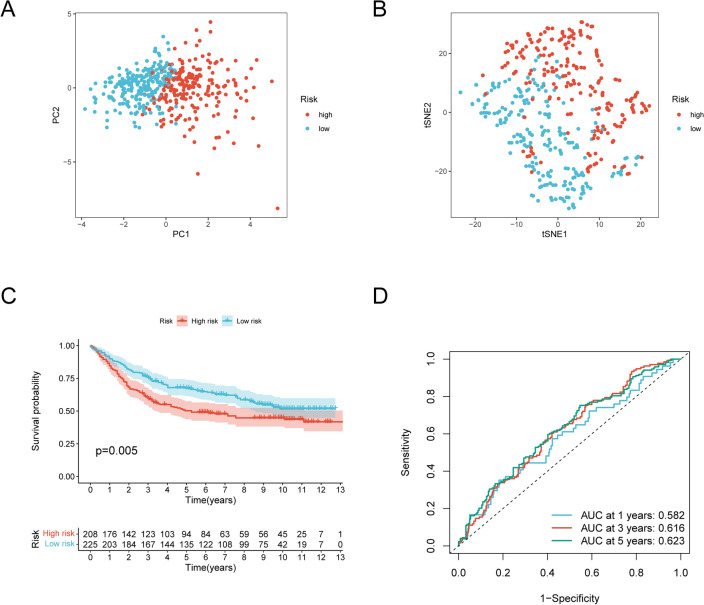
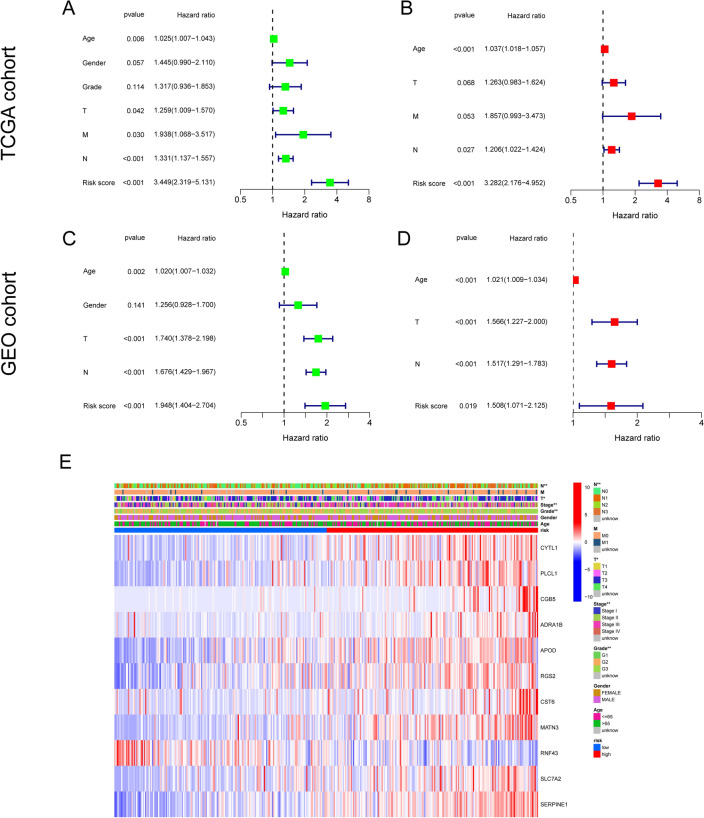
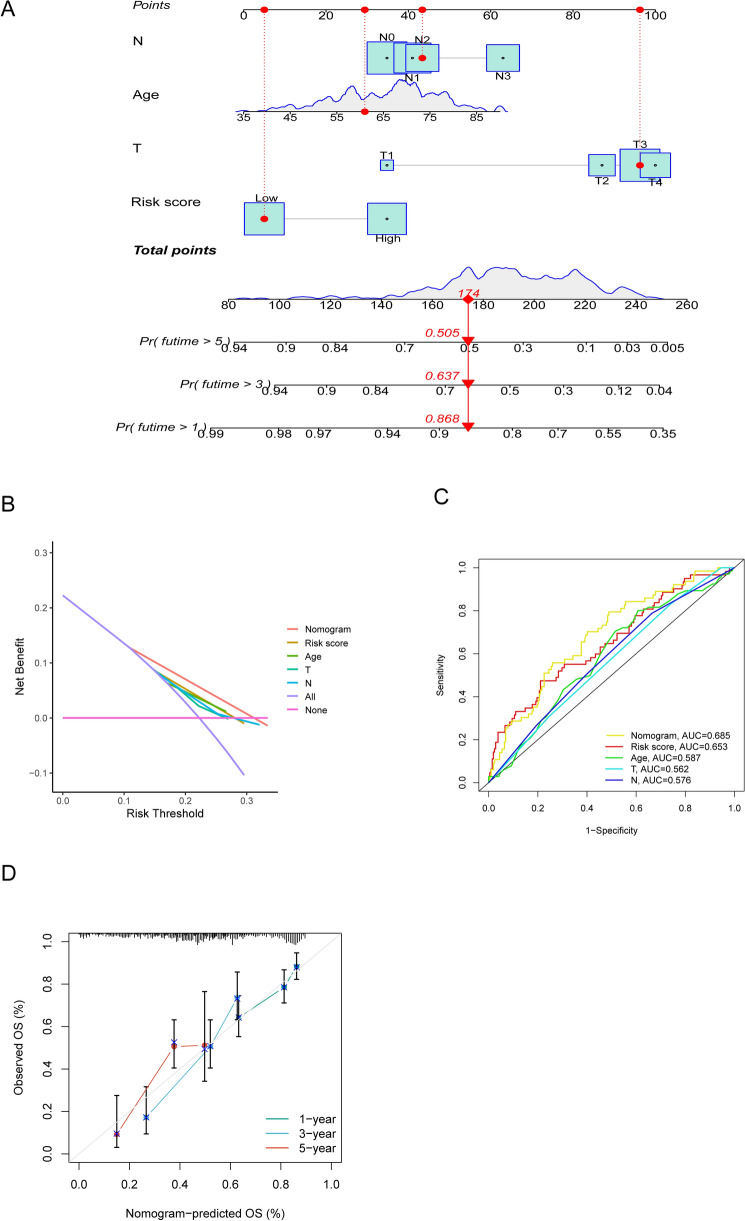
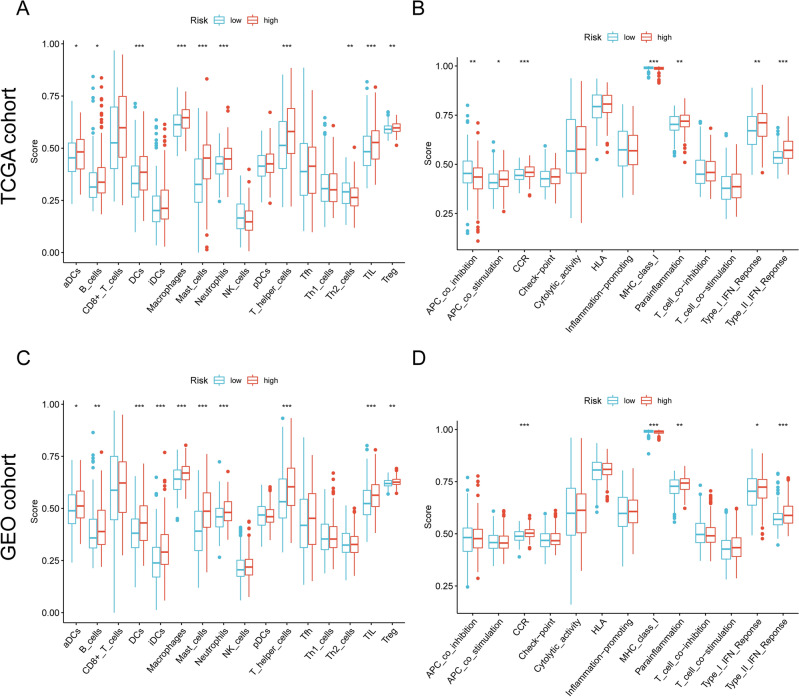
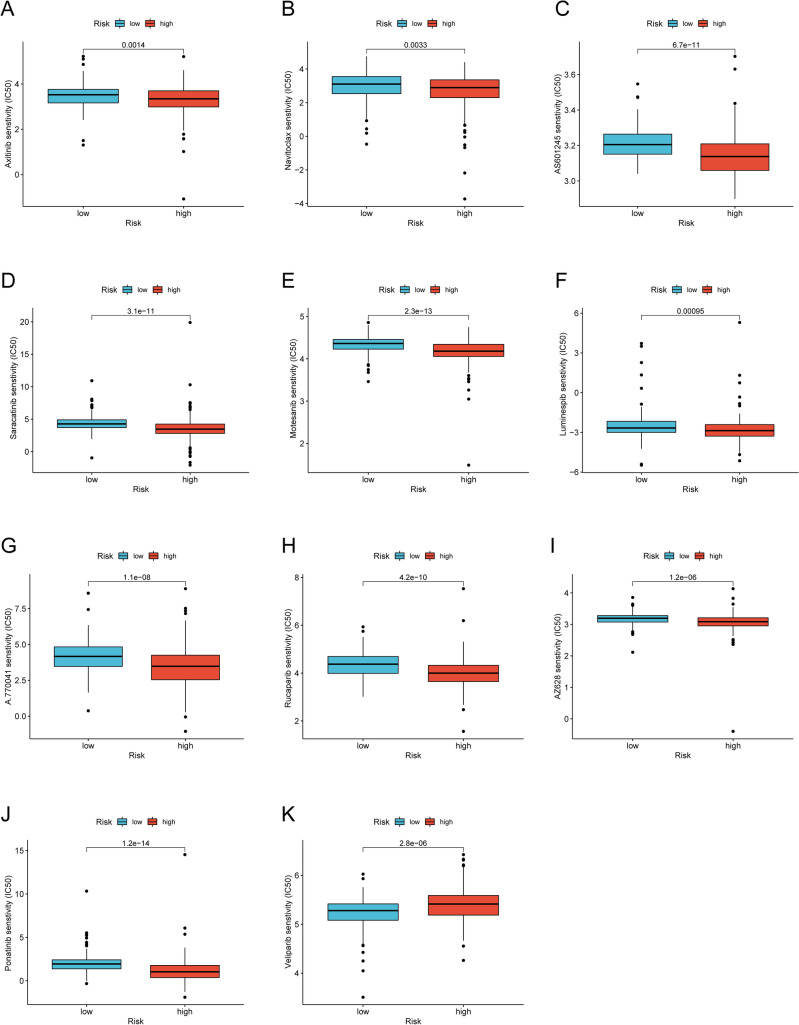
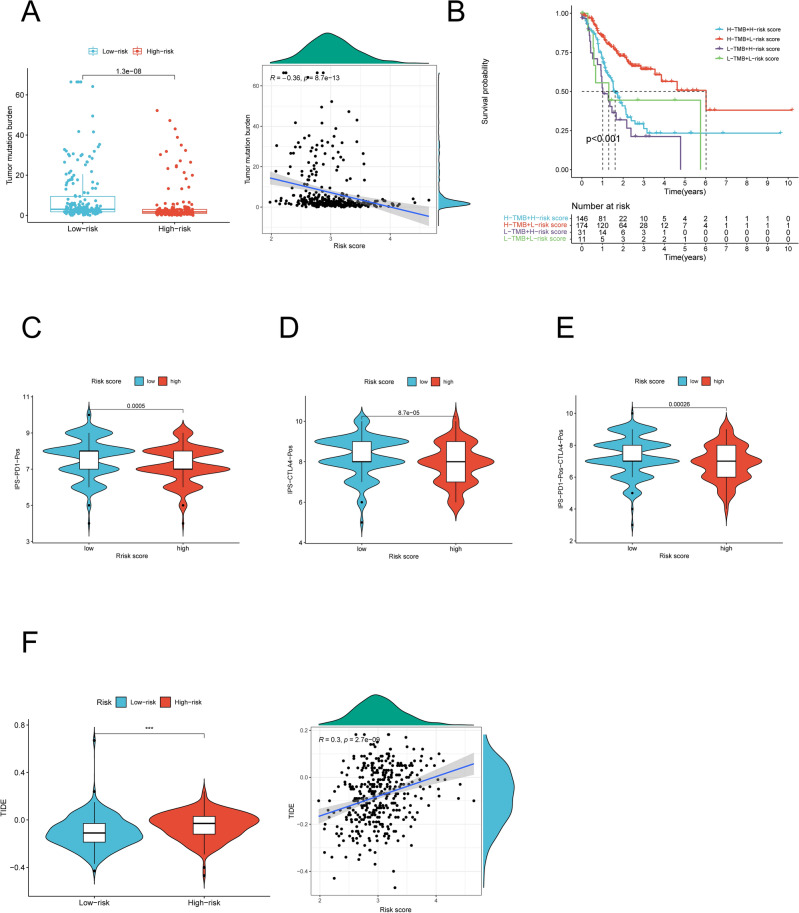
Necroptosis, a type of programmed cell death, has become a potential therapeutic target for solid tumors. Nevertheless, the potential roles of necroptosis-related genes (NRGs) in gastric cancer (GC) remain unknown. The objective of the present study was to create a necroptosis-related prognostic signature that can provide more accurate assessment of prognosis in GC. Using The Cancer Genome Atlas (TCGA) and Gene Expression Omnibus (GEO) data, we identified differentially expressed NRGs. Univariate analysis and Lasso regression were performed to determine the prognostic signature. Risk scores were calculated and all GC patients were divided into high- and low-risk score group according to the median risk score value. The robustness of this signature was externally validated with data from GSE84437 cohort (n = 431). Survival analysis revealed high-risk score patients had a worse prognosis. Results evidenced that the signature was an independent prognosis factor for survival. Single-sample sequence set enrichment analysis (ssGSEA) exhibited different enrichment of immune cells and immune-related pathways in the two risk groups. Furthermore, a predictive nomogram was generated and showed excellent predictive performance based on discrimination and calibration. In addition, the risk score positively correlated with tumor mutational burden and was associated with sensitivity to multiple anti-cancer drugs. Overall, our work demonstrates a close relationship between necroptosis and the prognosis of GC. The signature we constructed with potential clinical application value, can be used for prognosis prediction and being a potential therapeutic responses indicator in GC patients.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
A novel necroptosis-related gene index for predicting prognosis and a cold tumor immune microenvironment in stomach adenocarcinoma.Front Immunol. 2022 Oct 27;13:968165. doi: 10.3389/fimmu.2022.968165. eCollection 2022. Front Immunol. 2022. PMID: 36389725 Free PMC article. Review.
-
Construction and validation of a prognostic signature based on necroptosis-related genes in hepatocellular carcinoma.PLoS One. 2023 Feb 16;18(2):e0279744. doi: 10.1371/journal.pone.0279744. eCollection 2023. PLoS One. 2023. PMID: 36795724 Free PMC article.
-
Identification and validation of necroptosis-related prognostic gene signature and tumor immune microenvironment infiltration characterization in esophageal carcinoma.BMC Gastroenterol. 2022 Jul 15;22(1):344. doi: 10.1186/s12876-022-02423-6. BMC Gastroenterol. 2022. PMID: 35840882 Free PMC article.
-
Comprehensive Profiling Reveals Prognostic and Immunogenic Characteristics of Necroptosis in Soft Tissue Sarcomas.Front Immunol. 2022 May 18;13:877815. doi: 10.3389/fimmu.2022.877815. eCollection 2022. Front Immunol. 2022. PMID: 35663937 Free PMC article.
-
A necroptosis-related gene signature for predicting prognosis, immune landscape, and drug sensitivity in hepatocellular carcinoma.Cancer Med. 2022 Dec;11(24):5079-5096. doi: 10.1002/cam4.4812. Epub 2022 May 13. Cancer Med. 2022. PMID: 35560794 Free PMC article.
Cited by
-
Identification of molecular subtypes and a prognostic signature based on m6A/m5C/m1A-related genes in lung adenocarcinoma.Sci Rep. 2024 Mar 30;14(1):7543. doi: 10.1038/s41598-024-57910-5. Sci Rep. 2024. PMID: 38555384 Free PMC article.
-
Integrated Multi-omics Data Analysis and In Vitro Validation Reveal the Crucial Role of Glycogen Metabolism in Gastric Cancer.J Cancer. 2025 Jan 13;16(4):1243-1263. doi: 10.7150/jca.104424. eCollection 2025. J Cancer. 2025. PMID: 39895799 Free PMC article.
-
Bioinformatics Analysis of Biomarkers and Therapeutic Targets Related to Necroptosis in Intervertebral Disc Degeneration.Biomed Res Int. 2024 Dec 16;2024:9922966. doi: 10.1155/bmri/9922966. eCollection 2024. Biomed Res Int. 2024. PMID: 39717265 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
