

External validation of inpatient neonatal mortality prediction models in high-mortality settings
- PMID: 35918732
- PMCID: PMC9347100
- DOI: 10.1186/s12916-022-02439-5
External validation of inpatient neonatal mortality prediction models in high-mortality settings
Abstract
Background: Two neonatal mortality prediction models, the Neonatal Essential Treatment Score (NETS) which uses treatments prescribed at admission and the Score for Essential Neonatal Symptoms and Signs (SENSS) which uses basic clinical signs, were derived in high-mortality, low-resource settings to utilise data more likely to be available in these settings. In this study, we evaluate the predictive accuracy of two neonatal prediction models for all-cause in-hospital mortality.
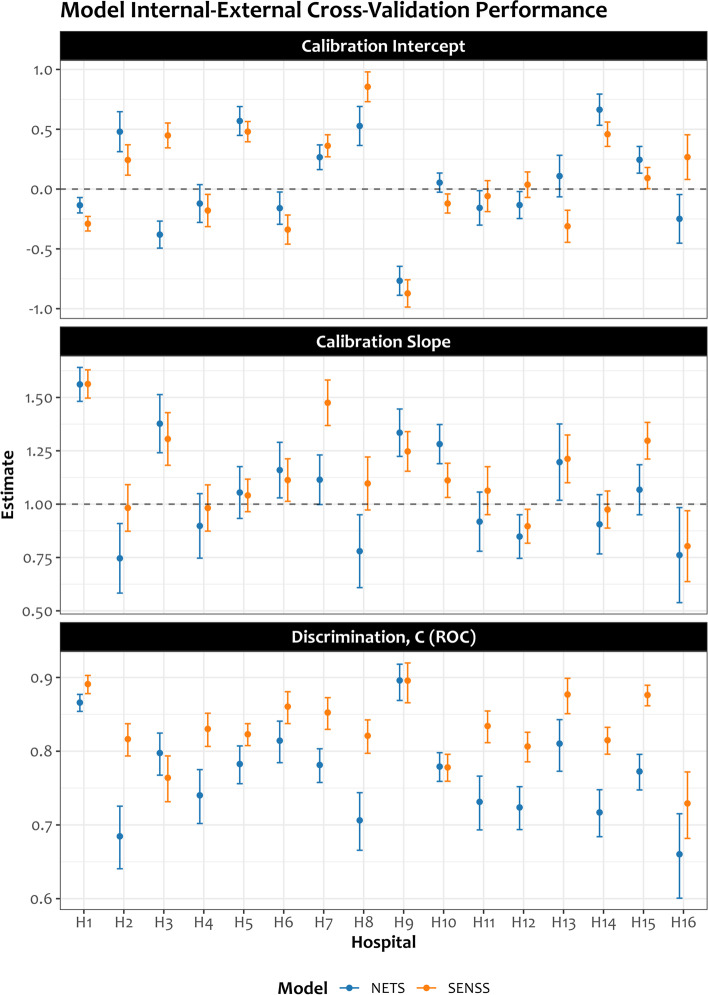
Methods: We used retrospectively collected routine clinical data recorded by duty clinicians at admission from 16 Kenyan hospitals used to externally validate and update the SENSS and NETS models that were initially developed from the data from the largest Kenyan maternity hospital to predict in-hospital mortality. Model performance was evaluated by assessing discrimination and calibration. Discrimination, the ability of the model to differentiate between those with and without the outcome, was measured using the c-statistic. Calibration, the agreement between predictions from the model and what was observed, was measured using the calibration intercept and slope (with values of 0 and 1 denoting perfect calibration).
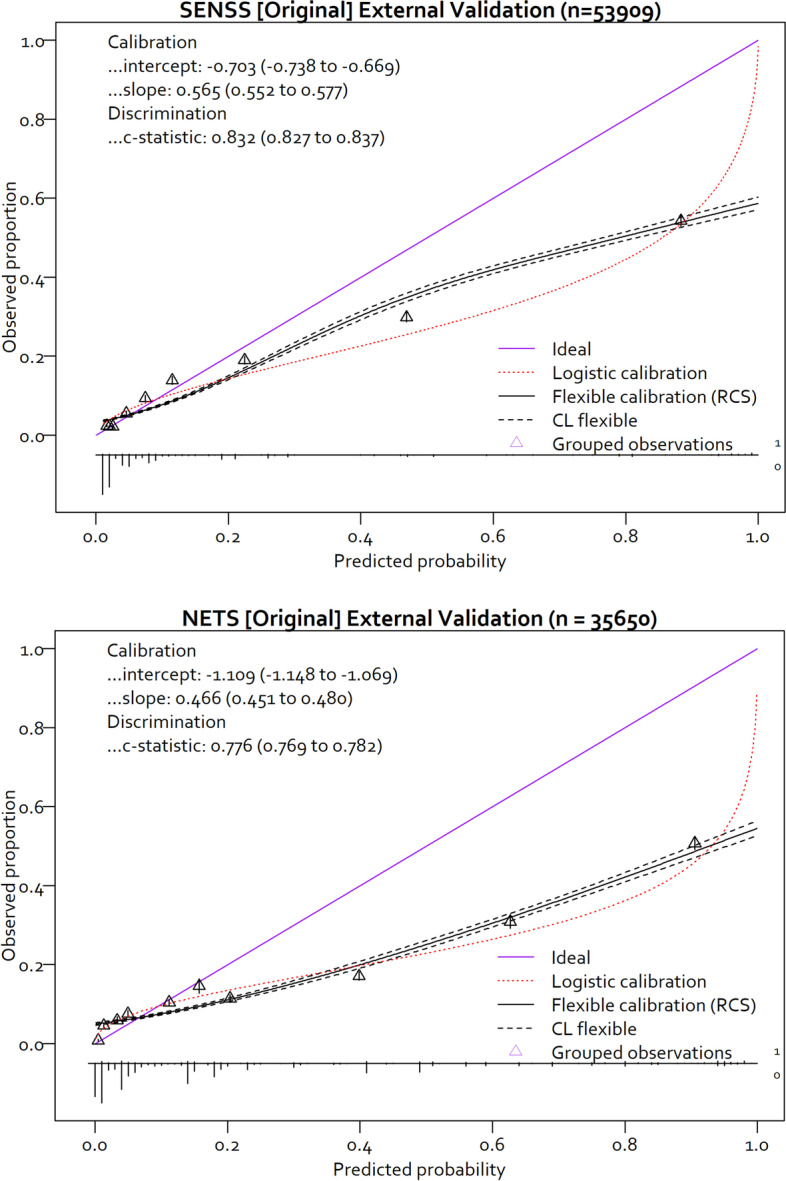
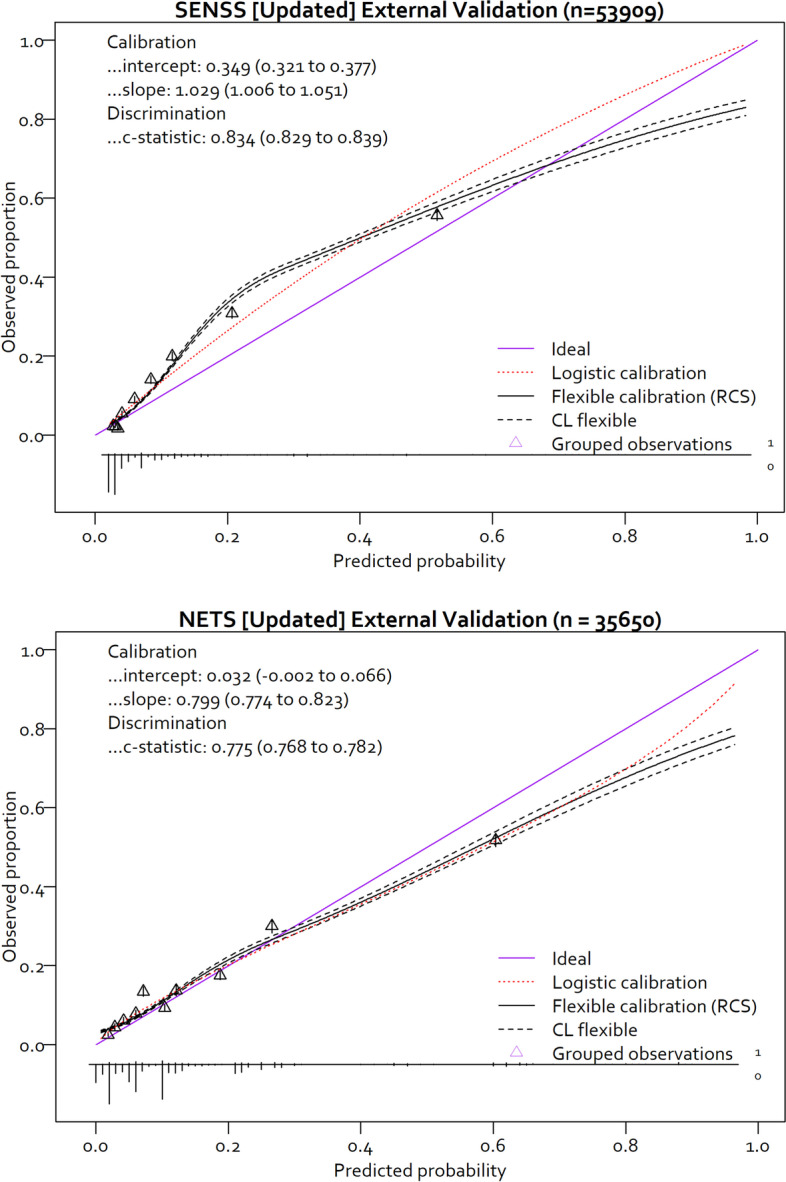
Results: At initial external validation, the estimated mortality risks from the original SENSS and NETS models were markedly overestimated with calibration intercepts of - 0.703 (95% CI - 0.738 to - 0.669) and - 1.109 (95% CI - 1.148 to - 1.069) and too extreme with calibration slopes of 0.565 (95% CI 0.552 to 0.577) and 0.466 (95% CI 0.451 to 0.480), respectively. After model updating, the calibration of the model improved. The updated SENSS and NETS models had calibration intercepts of 0.311 (95% CI 0.282 to 0.350) and 0.032 (95% CI - 0.002 to 0.066) and calibration slopes of 1.029 (95% CI 1.006 to 1.051) and 0.799 (95% CI 0.774 to 0.823), respectively, while showing good discrimination with c-statistics of 0.834 (95% CI 0.829 to 0.839) and 0.775 (95% CI 0.768 to 0.782), respectively. The overall calibration performance of the updated SENSS and NETS models was better than any existing neonatal in-hospital mortality prediction models externally validated for settings comparable to Kenya.
Conclusion: Few prediction models undergo rigorous external validation. We show how external validation using data from multiple locations enables model updating and improving their performance and potential value. The improved models indicate it is possible to predict in-hospital mortality using either treatments or signs and symptoms derived from routine neonatal data from low-resource hospital settings also making possible their use for case-mix adjustment when contrasting similar hospital settings.
Keywords: Africa; Hospital mortality; Newborn; Prognosis; Risk factors.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- United Nations General Assembly . Transforming our world: the 2030 agenda for sustainable development. 2016.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
