

Macrophages as a therapeutic target to promote diabetic wound healing
- PMID: 35918892
- PMCID: PMC9482022
- DOI: 10.1016/j.ymthe.2022.07.016
Macrophages as a therapeutic target to promote diabetic wound healing
Abstract
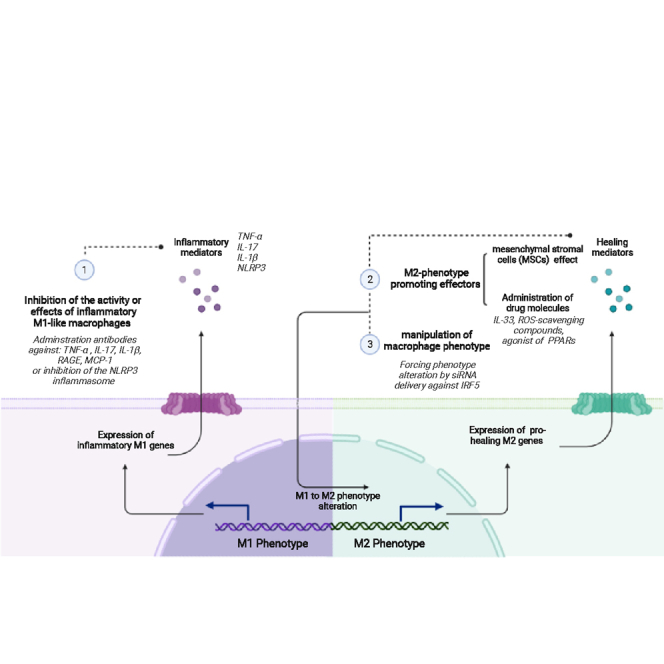
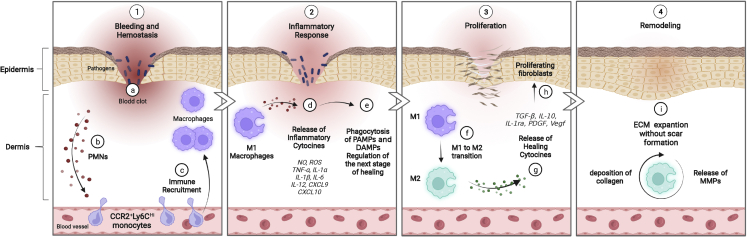
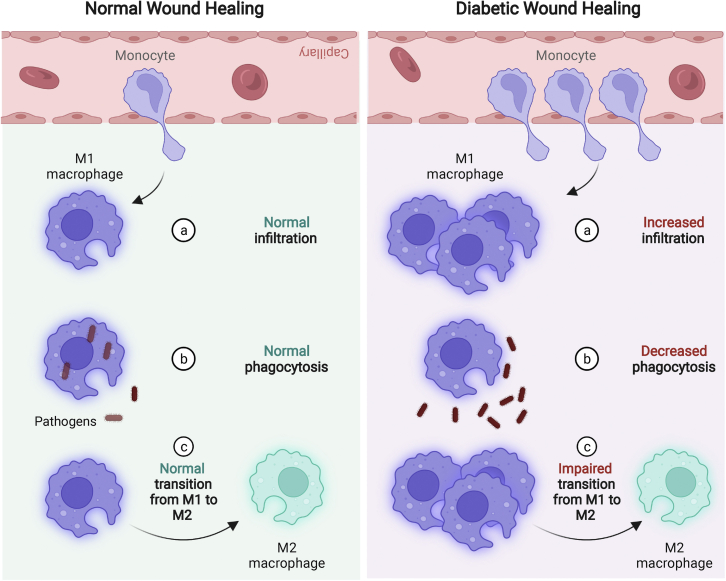
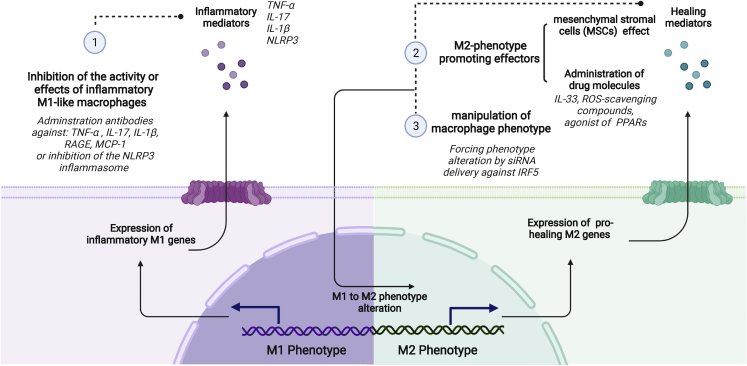
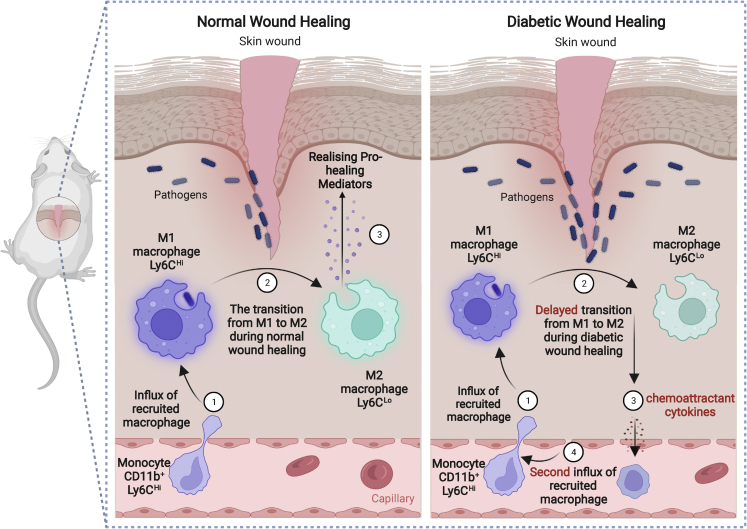
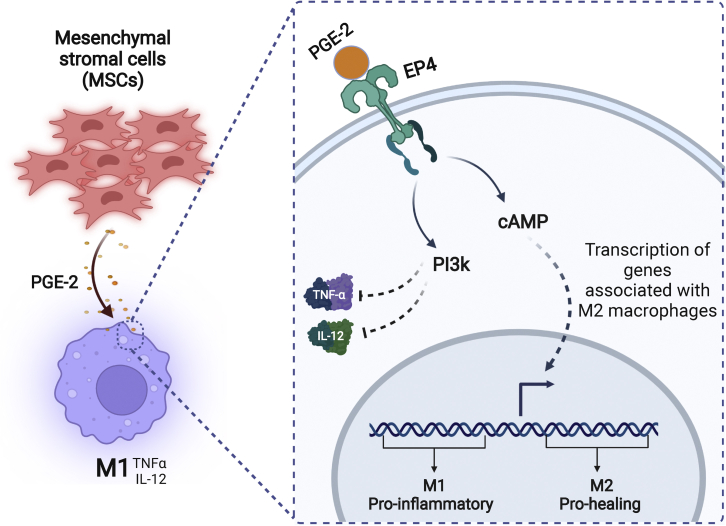
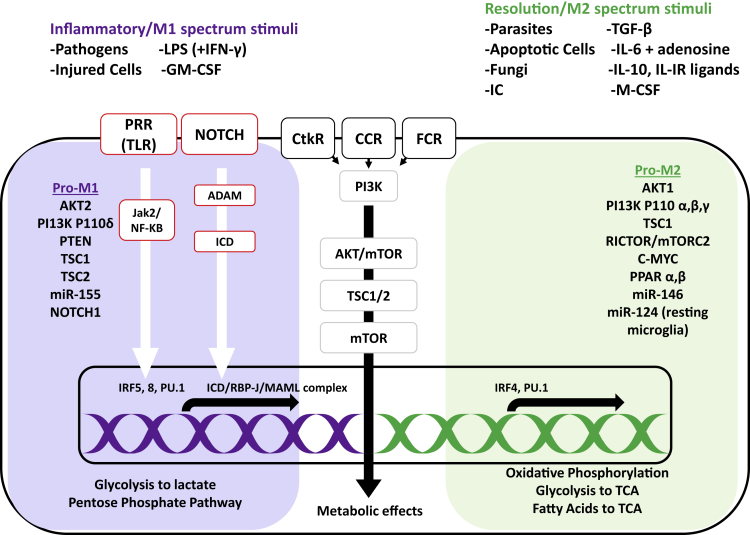
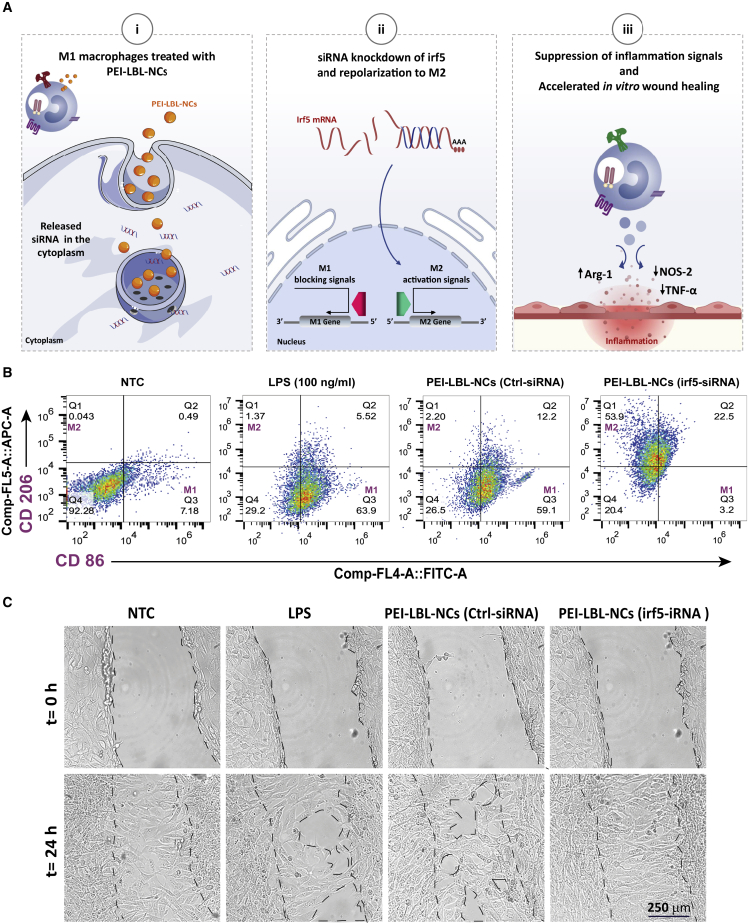
It is well established that macrophages are key regulators of wound healing, displaying impressive plasticity and an evolving phenotype, from an aggressive pro-inflammatory or "M1" phenotype to a pro-healing or "M2" phenotype, depending on the wound healing stage, to ensure proper healing. Because dysregulated macrophage responses have been linked to impaired healing of diabetic wounds, macrophages are being considered as a therapeutic target for improved wound healing. In this review, we first discuss the role of macrophages in a normal skin wound healing process and discuss the aberrations that occur in macrophages under diabetic conditions. Next we provide an overview of recent macrophage-based therapeutic approaches, including delivery of ex-vivo-activated macrophages and delivery of pharmacological strategies aimed at eliminating or re-educating local skin macrophages. In particular, we focus on strategies to silence key regulator genes to repolarize wound macrophages to the M2 phenotype, and we provide a discussion of their potential future clinical translation.
Keywords: IRF5; M1; M2; drug delivery; inflammation; macrophage; siRNA; wound healing.
Copyright © 2022 The American Society of Gene and Cell Therapy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
References
-
- Proksch E., Brandner J.M., Jensen J.M. The skin: an indispensable barrier. Exp. Dermatol. 2008;17:1063–1072. - PubMed
-
- Diegelmann R.F., Evans M.C. Wound healing: an overview of acute, fibrotic and delayed healing. Front. Biosci. 2004;9:283–289. - PubMed
-
- Gurtner G.C., Werner S., Barrandon Y., Longaker M.T. Wound repair and regeneration. Nature. 2008;453:314–321. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
